Authorization to Use and Disclose Protected Health Information - the Local Choice - Virginia
Authorization to Use and Disclose Protected Health Information - the Local Choice is a legal document that was released by the Virginia Department of Human Resource Management - a government authority operating within Virginia.
FAQ
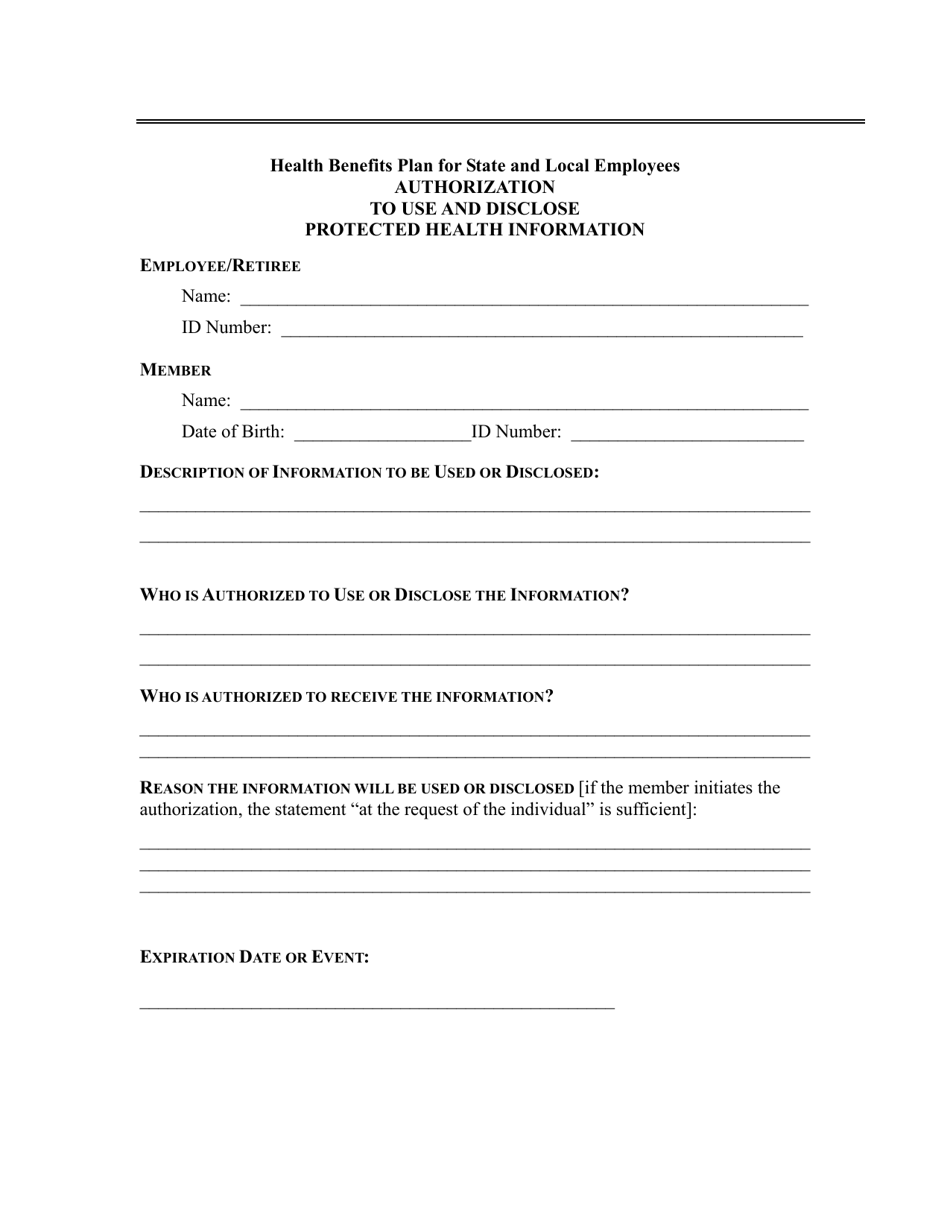
Q: What is the purpose of the Authorization to Use and Disclose Protected Health Information?
A: The purpose is to allow the release of a patient's health information to a specified individual or organization.
Q: What is Protected Health Information (PHI)?
A: PHI refers to any individually identifiable health information that is created or received by a healthcare provider, health plan, employer, or healthcare clearinghouse.
Q: Why do I need to sign an Authorization to Use and Disclose PHI?
A: You need to sign this authorization to give permission for your healthcare provider or health plan to share your health information with others.
Q: Who can request access to PHI with a signed authorization?
A: A signed authorization allows anyone specifically identified in the authorization to access and receive your PHI.
Q: Can I limit the information disclosed in an authorization?
A: Yes, you can specify the specific information you want to authorize for disclosure and any limitations on its use.
Q: Is there a time limit on how long an authorization is valid?
A: There is no expiration date specified in the Authorization to Use and Disclose PHI, but you can specify an expiration date or event in the authorization.
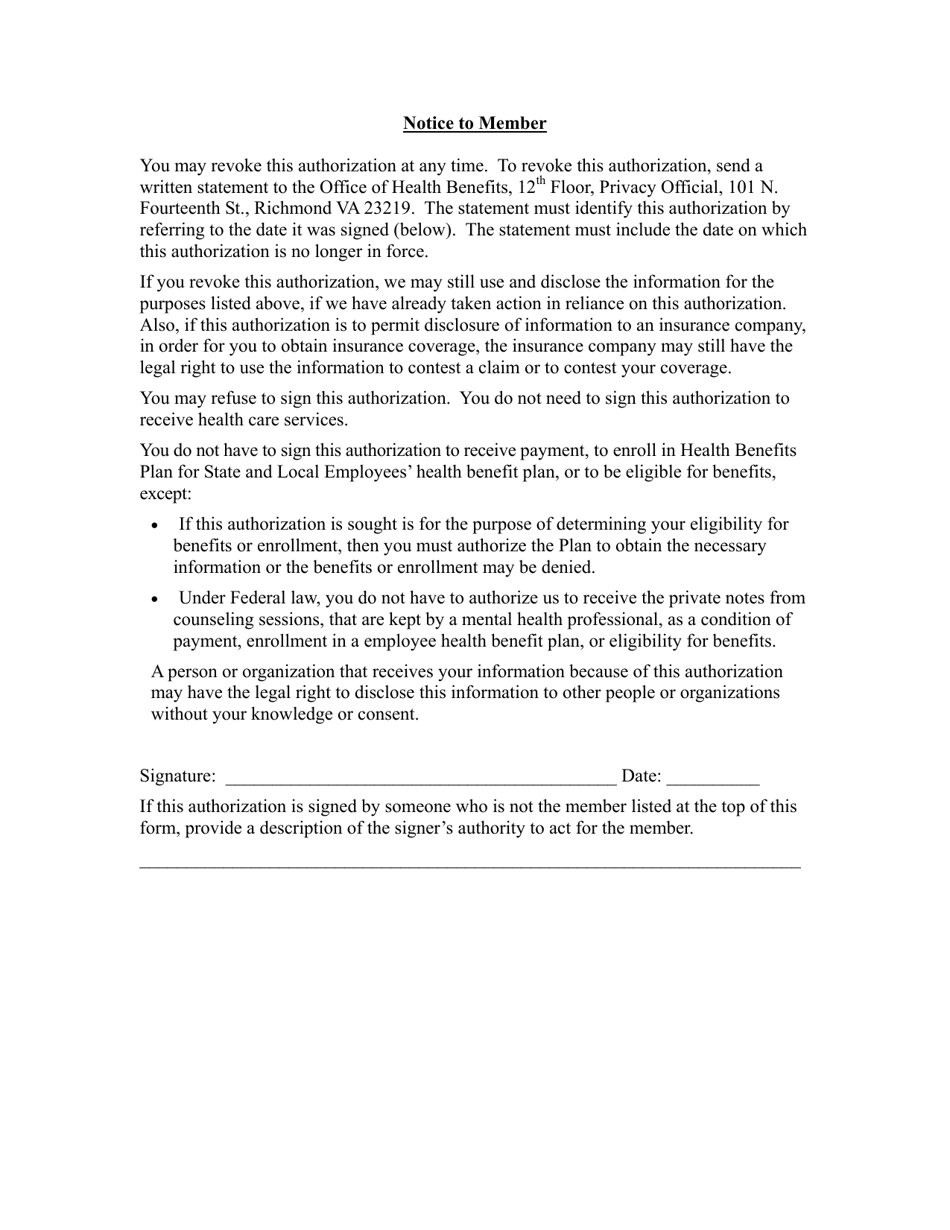
Q: Can I revoke an authorization?
A: Yes, you have the right to revoke an authorization at any time in writing.
Q: Are there any exceptions to the requirement for a signed authorization?
A: Yes, there are certain circumstances where a signed authorization is not required, such as for treatment, payment, or healthcare operations.
Q: What happens if my authorization is not accepted?
A: If your authorization is not accepted, your healthcare provider or health plan may not release your protected health information to the requested individual or organization.
Form Details:
- The latest edition currently provided by the Virginia Department of Human Resource Management;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Virginia Department of Human Resource Management.
Download Authorization to Use and Disclose Protected Health Information - the Local Choice - Virginia
1

2