Form SOC829 In-home Supportive Services (Ihss) / Waiver Personal Care Services (Wpcs) Provider Direct Deposit Enrollment / Change / Cancellation Form - California
What Is Form SOC829?
This is a legal form that was released by the California Department of Social Services - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form SOC829?
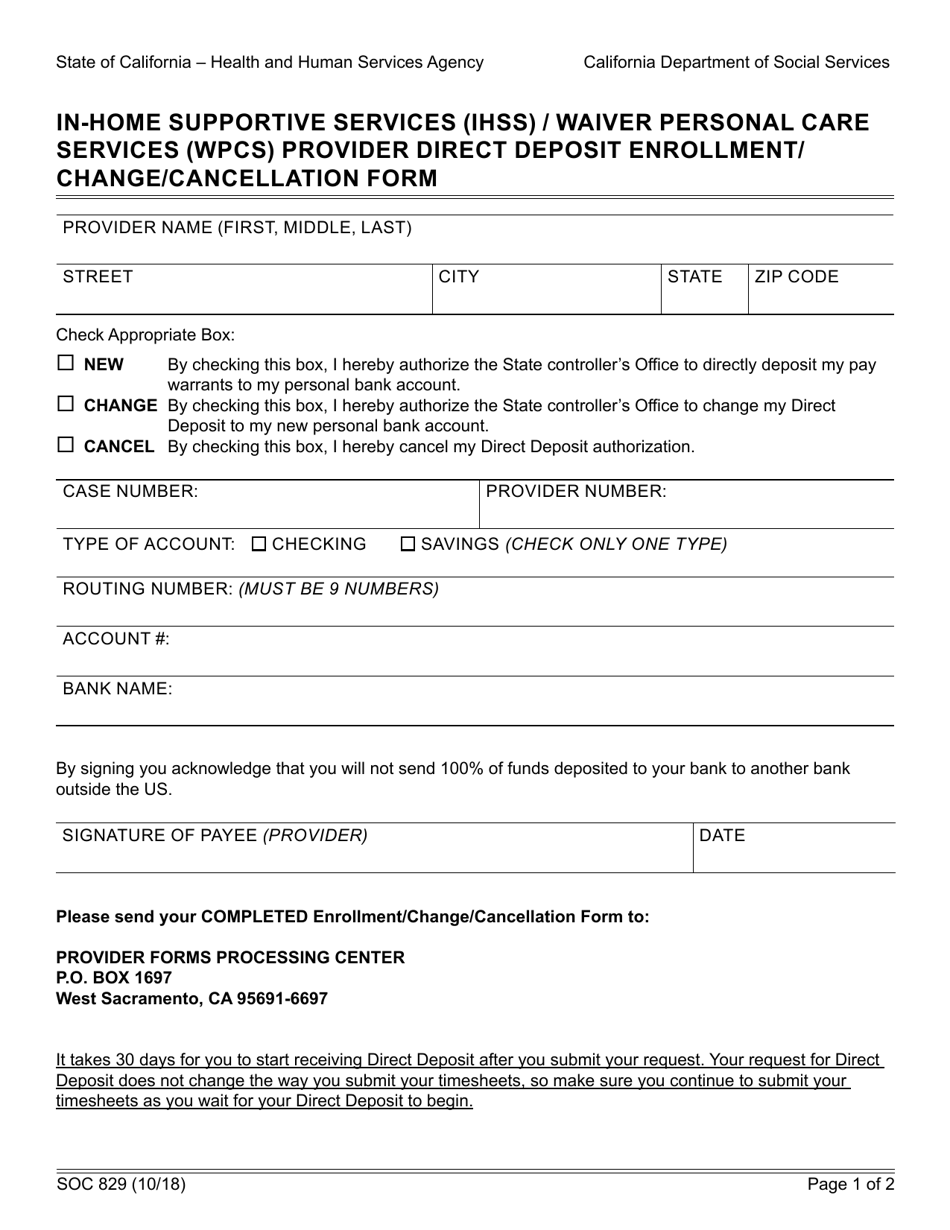
A: Form SOC829 is the In-home Supportive Services (IHSS)/Waiver Personal Care Services (WPCS) Provider Direct Deposit Enrollment/Change/Cancellation Form in California.
Q: What is IHSS?
A: IHSS stands for In-home Supportive Services.
Q: What is WPCS?
A: WPCS stands for Waiver Personal Care Services.
Q: What is the purpose of Form SOC829?
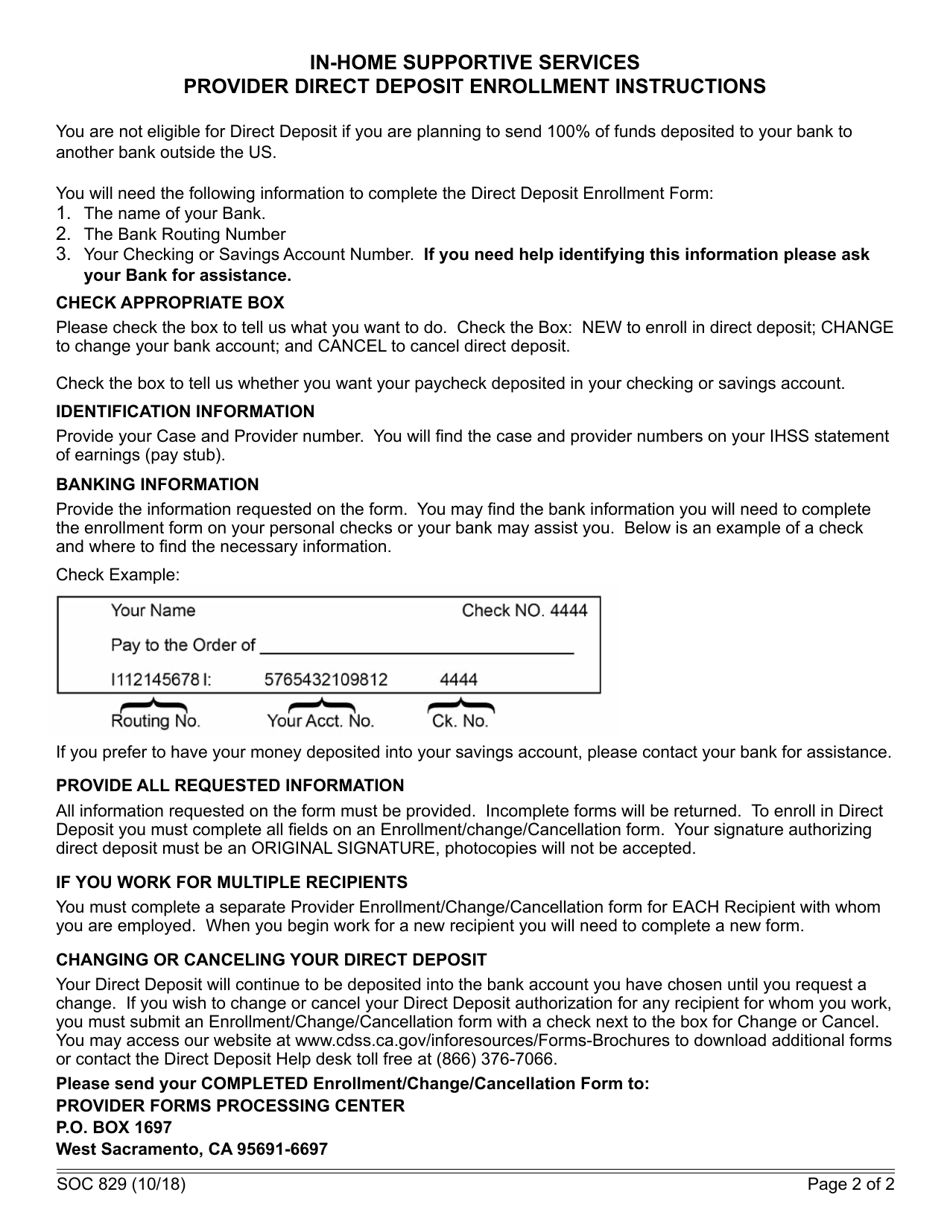
A: The purpose of Form SOC829 is to enroll, change, or cancel direct deposit for IHSS/WPCS provider payments.
Q: Who needs to fill out Form SOC829?
A: IHSS/WPCS providers in California need to fill out Form SOC829.
Q: What information is required in Form SOC829?
A: Form SOC829 requires information such as provider name, provider number, bank account details, and signature.
Q: Can Form SOC829 be used for other states?
A: No, Form SOC829 is specific to California and cannot be used for other states.
Q: Is there a fee for submitting Form SOC829?
A: No, there is no fee for submitting Form SOC829.
Q: How long does it take to process Form SOC829?
A: Processing times may vary, but it is recommended to allow at least 10 business days for the form to be processed.
Form Details:
- Released on October 1, 2018;
- The latest edition provided by the California Department of Social Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form SOC829 by clicking the link below or browse more documents and templates provided by the California Department of Social Services.
Download Form SOC829 In-home Supportive Services (Ihss) / Waiver Personal Care Services (Wpcs) Provider Direct Deposit Enrollment / Change / Cancellation Form - California
1
2