![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM01913
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM01913
for the current year.
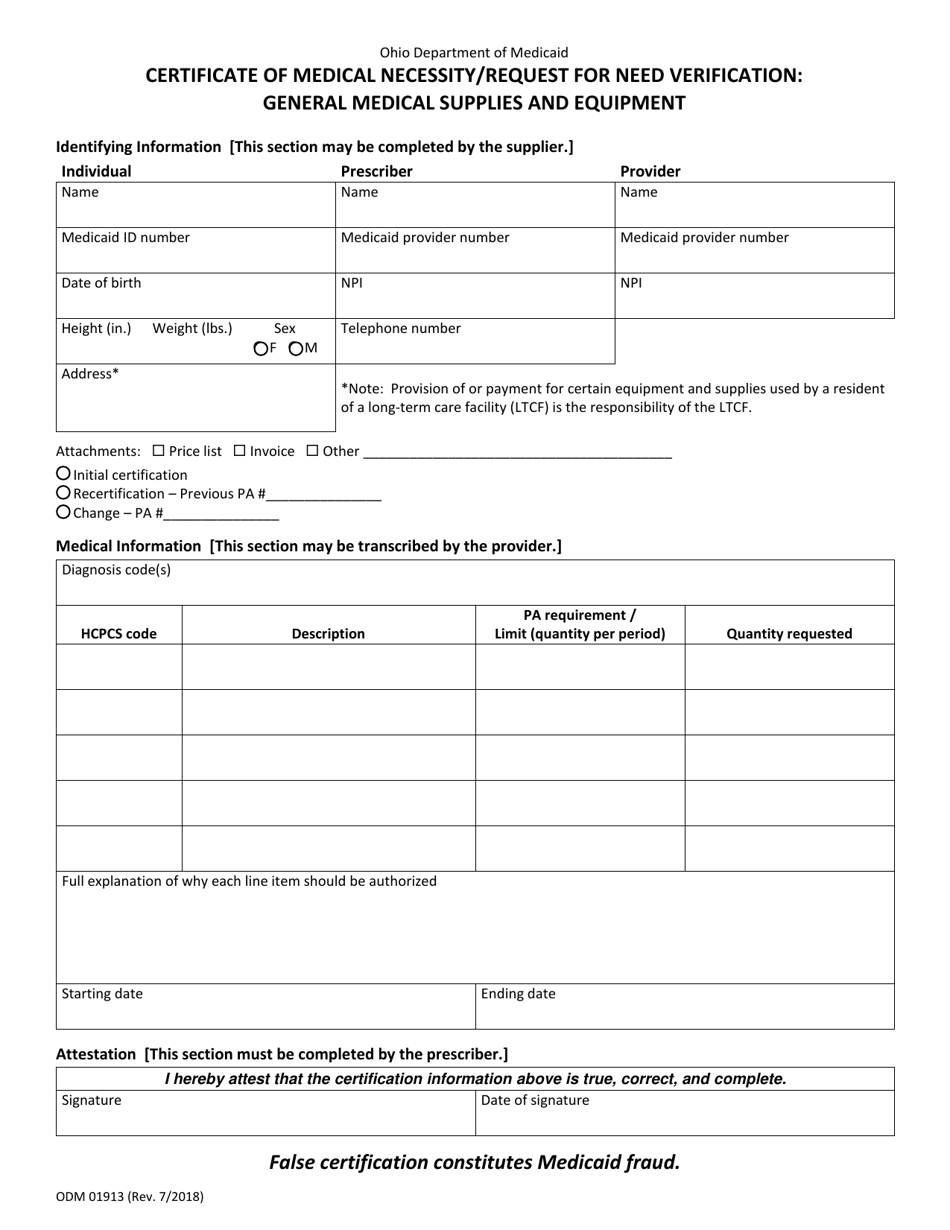
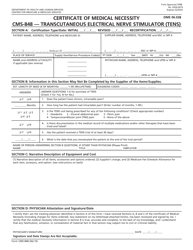
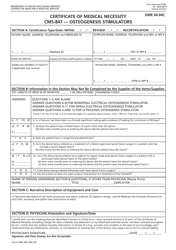
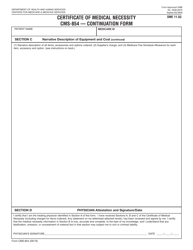
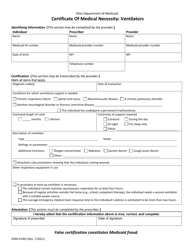
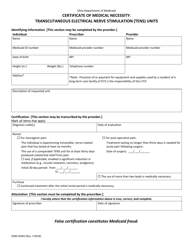
Form ODM01913 Certificate of Medical Necessity / Request for Need Verification - General Medical Supplies and Equipment - Ohio
What Is Form ODM01913?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is ODM01913 Certificate of Medical Necessity/Request for Need Verification?
A: ODM01913 is a form used in Ohio to request verification of medical necessity for general medical supplies and equipment.
Q: Who uses the ODM01913 form?
A: The ODM01913 form is used by individuals who need general medical supplies and equipment and are seeking verification of medical necessity in Ohio.
Q: What is the purpose of the ODM01913 form?
A: The purpose of the ODM01913 form is to provide necessary information and documentation to justify the need for general medical supplies and equipment.
Q: What information is required on the ODM01913 form?
A: The ODM01913 form requires information such as the patient's personal details, healthcare provider information, description of the medical supplies or equipment being requested, and supporting documentation from healthcare professionals.
Q: What is the process after submitting the ODM01913 form?
A: After submitting the ODM01913 form, it will be reviewed by the Ohio Department of Medicaid or an authorized agency to determine if the medical supplies and equipment are medically necessary. Approval or denial will be communicated to the individual or their healthcare provider.
Q: Can the ODM01913 form be used for all types of medical supplies and equipment?
A: The ODM01913 form is specifically for general medical supplies and equipment. Specialized or unique items may require different forms or documentation.
Q: Are there any fees associated with submitting the ODM01913 form?
A: Fees may vary depending on the specific medical supplies and equipment being requested and the individual's insurance coverage. It is advisable to check with the Ohio Department of Medicaid or the healthcare provider for information on any applicable fees.
Form Details:
- Released on July 1, 2018;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM01913 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.