![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM03199
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM03199
for the current year.
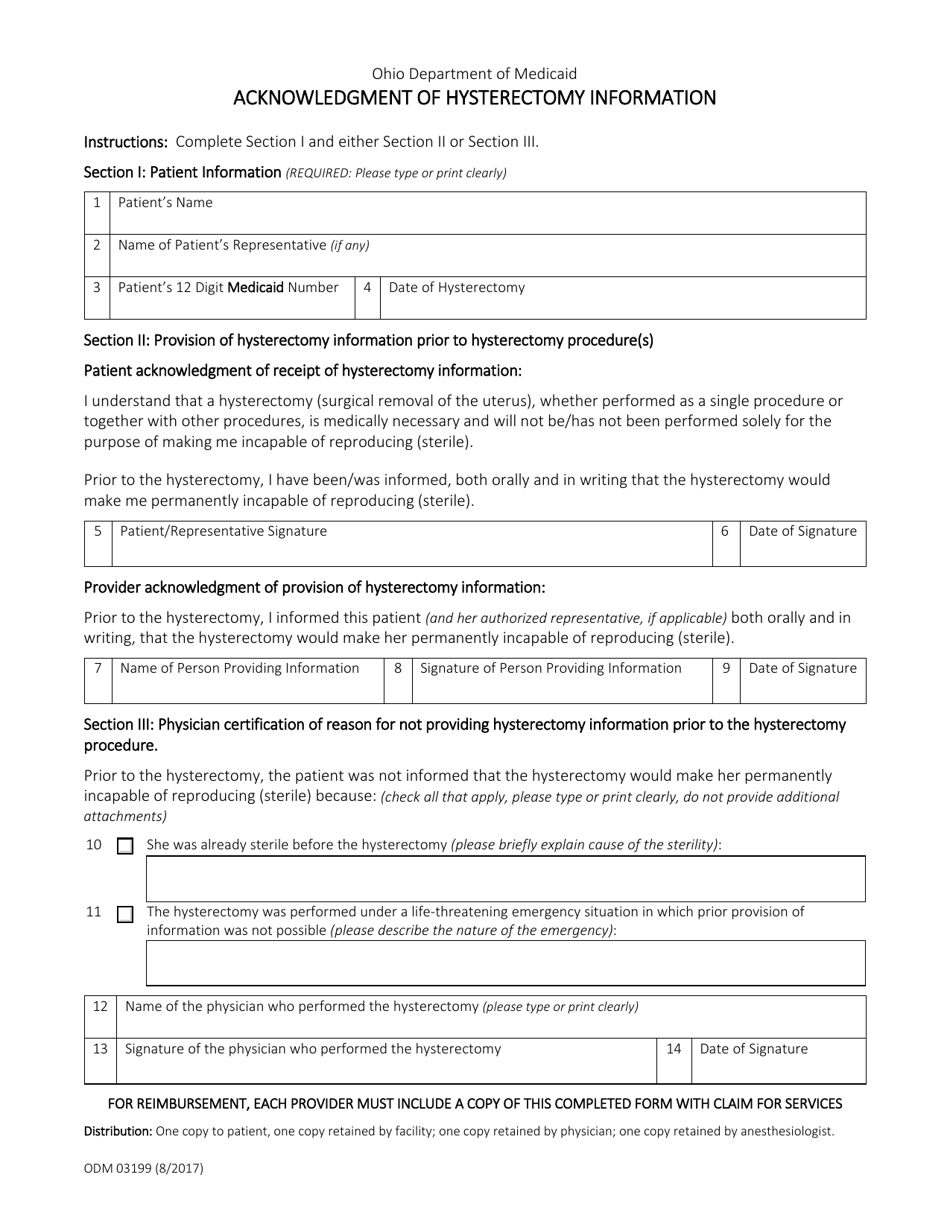
Form ODM03199 Acknowledgment of Hysterectomy Information - Ohio
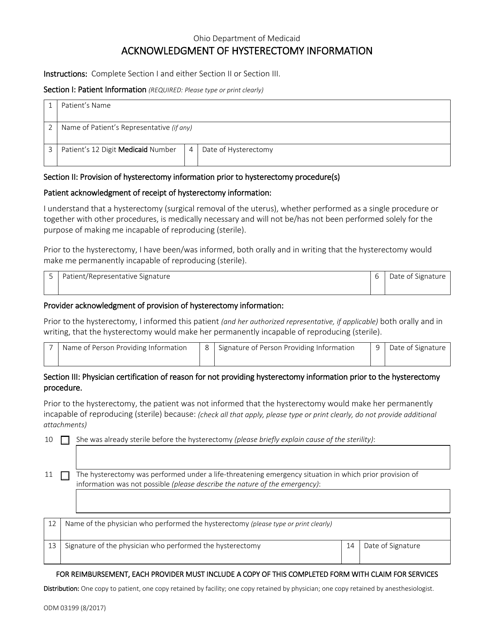
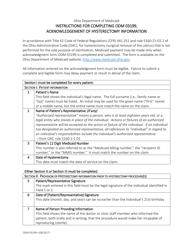
What Is Form ODM03199?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. Check the official instructions before completing and submitting the form.
FAQ
Q: What is Form ODM03199?
A: Form ODM03199 is the Acknowledgment of Hysterectomy Information form in Ohio.
Q: What is the purpose of Form ODM03199?
A: The purpose of this form is to receive acknowledgment from the patient that they have received and understood the information regarding hysterectomy procedures.
Q: When is Form ODM03199 used?
A: This form is used when a patient is undergoing a hysterectomy procedure in Ohio.
Q: Who needs to fill out Form ODM03199?
A: The patient undergoing a hysterectomy procedure needs to fill out this form.
Q: Do I need to keep a copy of Form ODM03199?
A: It is recommended to keep a copy of this form for your records.
Form Details:
- Released on August 1, 2017;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Available in Spanish;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM03199 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.