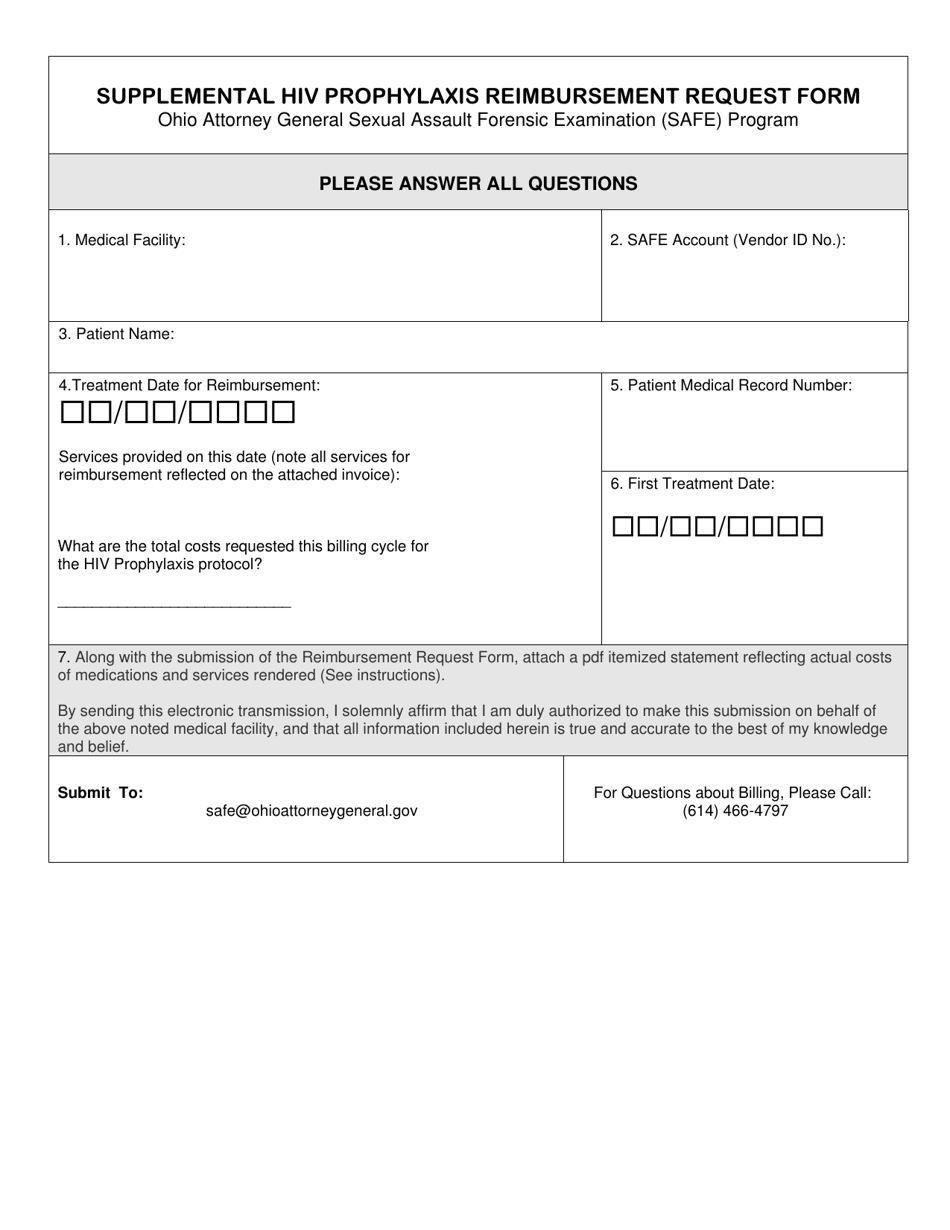
Supplemental HIV Prophylaxis Reimbursement Request Form - Ohio Attorney General Sexual Assault Forensic Examination (Safe) Program - Ohio
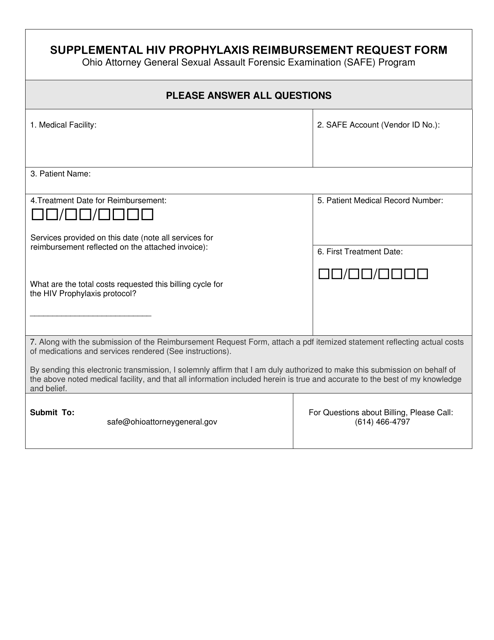
Supplemental HIV Prophylaxis Reimbursement Request Form - Ohio Attorney General Forensic Examination (Safe) Program is a legal document that was released by the Ohio Attorney General - a government authority operating within Ohio.
FAQ
Q: What is the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: The Supplemental HIV Prophylaxis Reimbursement Request Form is a form used for requesting reimbursement under the Ohio Attorney General Sexual Assault Forensic Examination (SAFE) Program.
Q: What is the Ohio Attorney General Sexual Assault Forensic Examination (SAFE) Program?
A: The Ohio Attorney General Sexual Assault Forensic Examination (SAFE) Program provides funding to healthcare providers and facilities for conducting sexual assault forensic examinations.
Q: Who is eligible to use the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: Healthcare providers and facilities participating in the Ohio Attorney General Sexual Assault Forensic Examination (SAFE) Program are eligible to use the Supplemental HIV Prophylaxis Reimbursement Request Form.
Q: What is the purpose of the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: The purpose of the form is to request reimbursement for the cost of providing supplemental HIV prophylaxis medications to sexual assault survivors.
Q: How can healthcare providers and facilities obtain the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: The form can be obtained through the Ohio Attorney General's Office or the Ohio Sexual Assault Nurse Examiner (SANE) Program.
Q: What information is required on the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: The form requires information such as the survivor's demographics, pharmacy information, prescription details, and the healthcare provider's information.
Q: Is there a deadline for submitting the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: Yes, the form must be submitted within 30 days of providing the HIV prophylaxis medications to the survivor.
Q: Is there a limit to the reimbursement amount for HIV prophylaxis medications?
A: Yes, the reimbursement amount is capped at $1,000 per survivor.
Q: Who should healthcare providers and facilities contact for further information about the Supplemental HIV Prophylaxis Reimbursement Request Form?
A: They should contact the Ohio Sexual Assault Nurse Examiner (SANE) Program or the Ohio Attorney General's Office for further information.
Form Details:
- The latest edition currently provided by the Ohio Attorney General;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Ohio Attorney General.