Form DOH-5247RU Medicaid Authorized Representative Designation / Change Request - New York (Russian)
This is a legal form that was released by the New York State Department of Health - a government authority operating within New York.
The document is provided in Russian. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
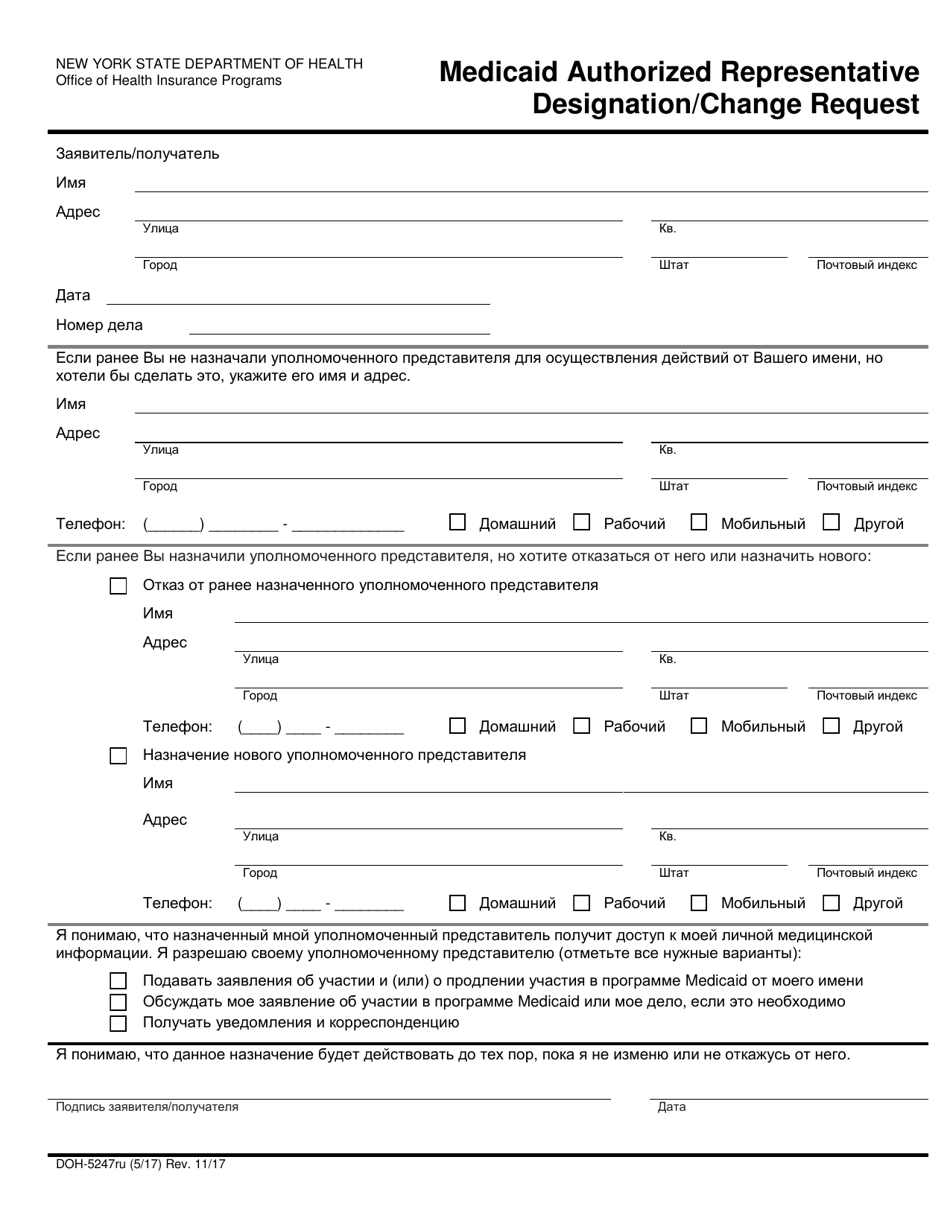
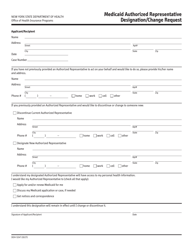
Q: What is Form DOH-5247RU?
A: Form DOH-5247RU is the Medicaid Authorized Representative Designation/Change Request form.
Q: What is the purpose of Form DOH-5247RU?
A: The purpose of Form DOH-5247RU is to designate or change an authorized representative for Medicaid in New York.
Q: Who can use Form DOH-5247RU?
A: Any Medicaid recipient in New York who wants to designate or change an authorized representative can use Form DOH-5247RU.
Q: What information is required on Form DOH-5247RU?
A: Form DOH-5247RU requires information about the Medicaid recipient, the authorized representative being designated or changed, and the reason for the designation or change.
Q: Is Form DOH-5247RU available in Russian?
A: Yes, Form DOH-5247RU is available in Russian.
Form Details:
- Released on November 1, 2017;
- The latest edition provided by the New York State Department of Health;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
Download a fillable version of Form DOH-5247RU by clicking the link below or browse more documents and templates provided by the New York State Department of Health.