![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM01959
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM01959
for the current year.
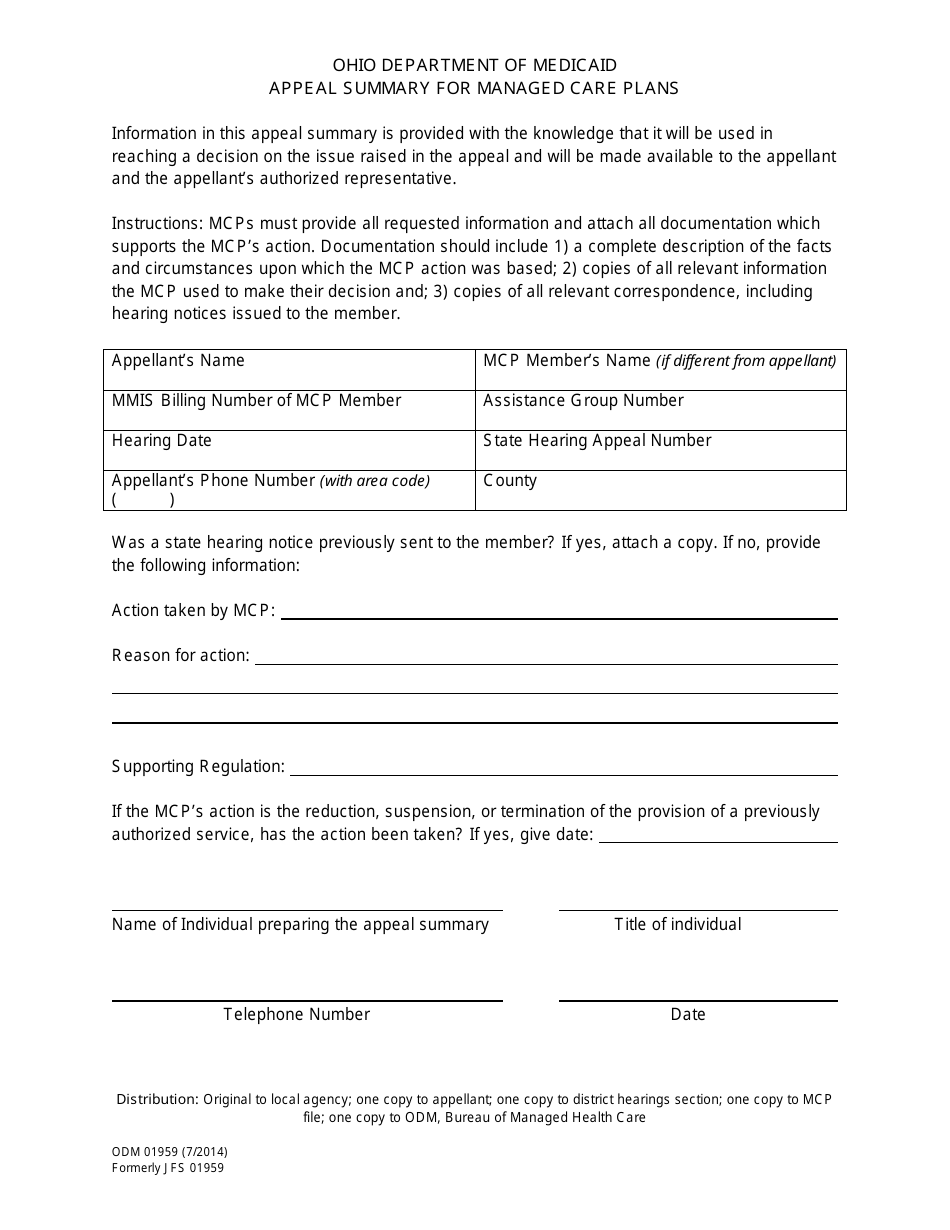
Form ODM01959 Appeal Summary for Managed Care Plans - Ohio
What Is Form ODM01959?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is ODM01959?
A: ODM01959 is an Appeal Summary for Managed Care Plans in Ohio.
Q: What is an appeal?
A: An appeal is a request for a review of a decision made by a managed care plan in Ohio.
Q: Who can file an appeal?
A: Any enrollee or their authorized representative can file an appeal.
Q: How do I file an appeal?
A: To file an appeal, you should follow the instructions provided in ODM01959 and submit it to the appropriate managed care plan.
Q: What information should be included in the appeal?
A: The appeal should include your name, contact information, the reason for the appeal, and any supporting documentation.
Q: Can I have assistance in filing an appeal?
A: Yes, you can seek assistance from an advocate or other authorized representative in filing an appeal.
Q: What happens after I file an appeal?
A: The managed care plan will review your appeal and make a decision. You will be notified of the outcome.
Q: What if I disagree with the decision made by the managed care plan?
A: If you disagree with the decision, you have the right to request a State Fair Hearing.
Q: Is there a deadline for filing an appeal?
A: Yes, there is a deadline for filing an appeal. Please refer to ODM01959 for the specific deadline for your case.
Form Details:
- Released on July 1, 2014;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM01959 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.