![]() This version of the form is not currently in use and is provided for reference only. Download this version of
VA Form 10-5345
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
VA Form 10-5345
for the current year.
VA Form 10-5345 Request for and Authorization to Release Health Information
What Is VA Form 10-5345?
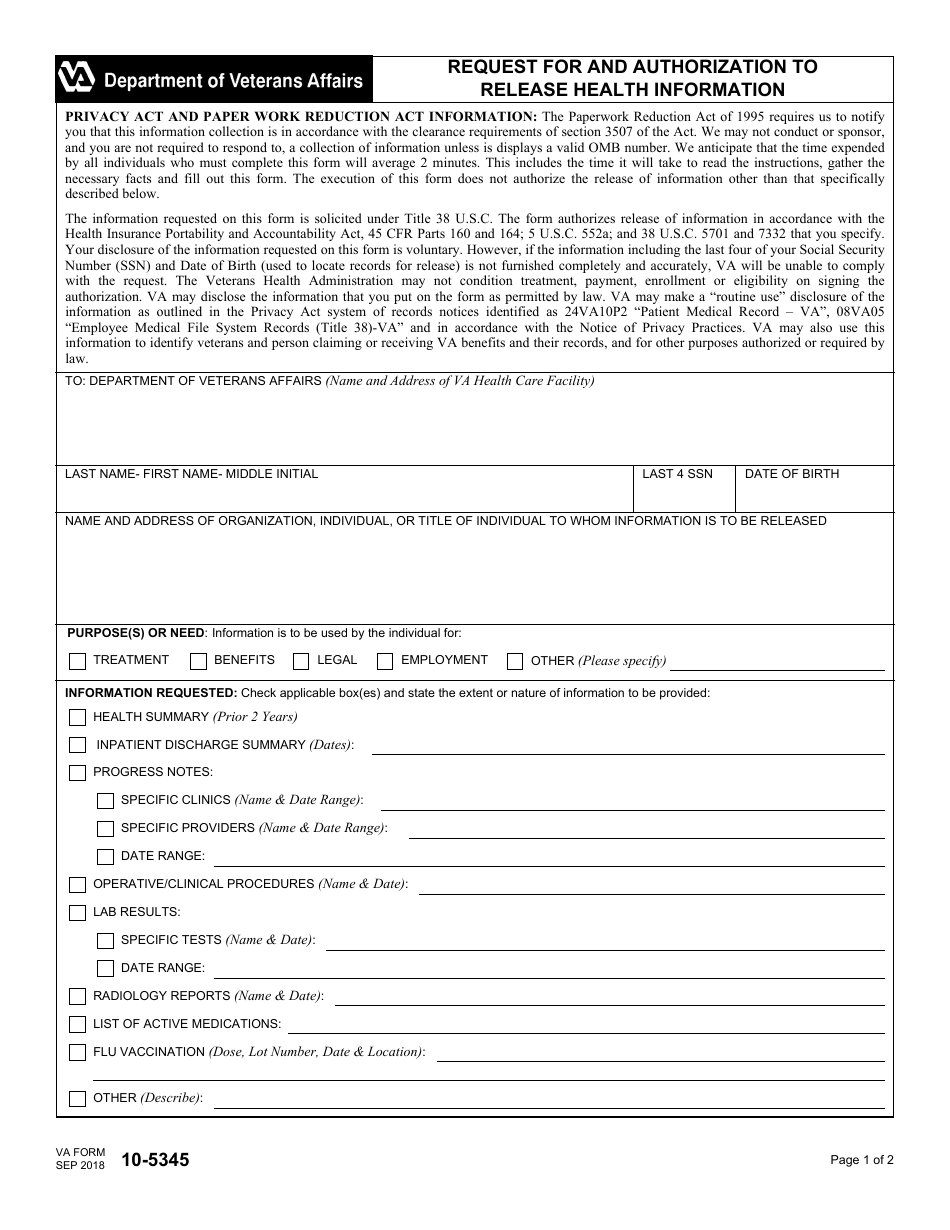
VA Form 10-5345, Request for and Authorization to Release Health Information , is a document used for getting a veteran's written and signed authorization to release their medical data according to the Health Insurance Portability and Accountability Act. The U.S. Department of Veterans Affairs (VA) may also apply the details provided in this paper to identify the individuals claiming or receiving any VA benefits.
The latest version of the form was released on September 1, 2018 . An up-to-date fillable version of the form is available for download below or can be found on the VA website. You are required to submit your request to VA if you need to disclose your medical data to any individual or organization for treatment, employment, legal or other purposes. You must fill out this document when submitting an application for VA benefits.
Related forms include VA Form 10-5345A, Individuals' Request for a Copy of Their Own Health Information, used for requesting a copy of a health record maintained by the VA and VA Form 10-5345A-MHV, Individual's Request for Med Record from MyHealtheVet, used to request a copy of a medical record through a MyHealtheVet account
VA Form 10-5345 Instructions
VA Form 10-5345 instructions are the following:
- The document must contain accurate and complete information;
- Though the disclosure of the data is voluntary, VA will not be able to process the request if the last four digits of your Social Security number (SSN) and your date of birth will be provided;
- The authorization can be recalled at any time;
- To recall the authorization, it is necessary to submit the corresponding written request. Verbal revocations are not accepted;
- After completing and signing the VA 10-5345, you will receive a copy of the form. It is required to keep this copy for references; and
- If you are not able to request the release of medical records, it can be done by your legal representative.
The data provided via this document may be re-disclosed to the same recipient.
How to Fill Out VA Form 10-5345?
The document consists of two pages. Most of its fields are self-explanatory. The average time needed to complete the document is about 2 minutes. The VA 10-5345 should be completed as follows:
- Enter the name and address of the VA healthcare facility.
- Indicate the name and address of the organization or individual to whom medical records are to be released.
- Specify the purpose for data disclosure.
- Specify the information you want to release in the "Information Requested" section. Check the appropriate boxes and provide details on the date range and nature of the information to be disclosed.
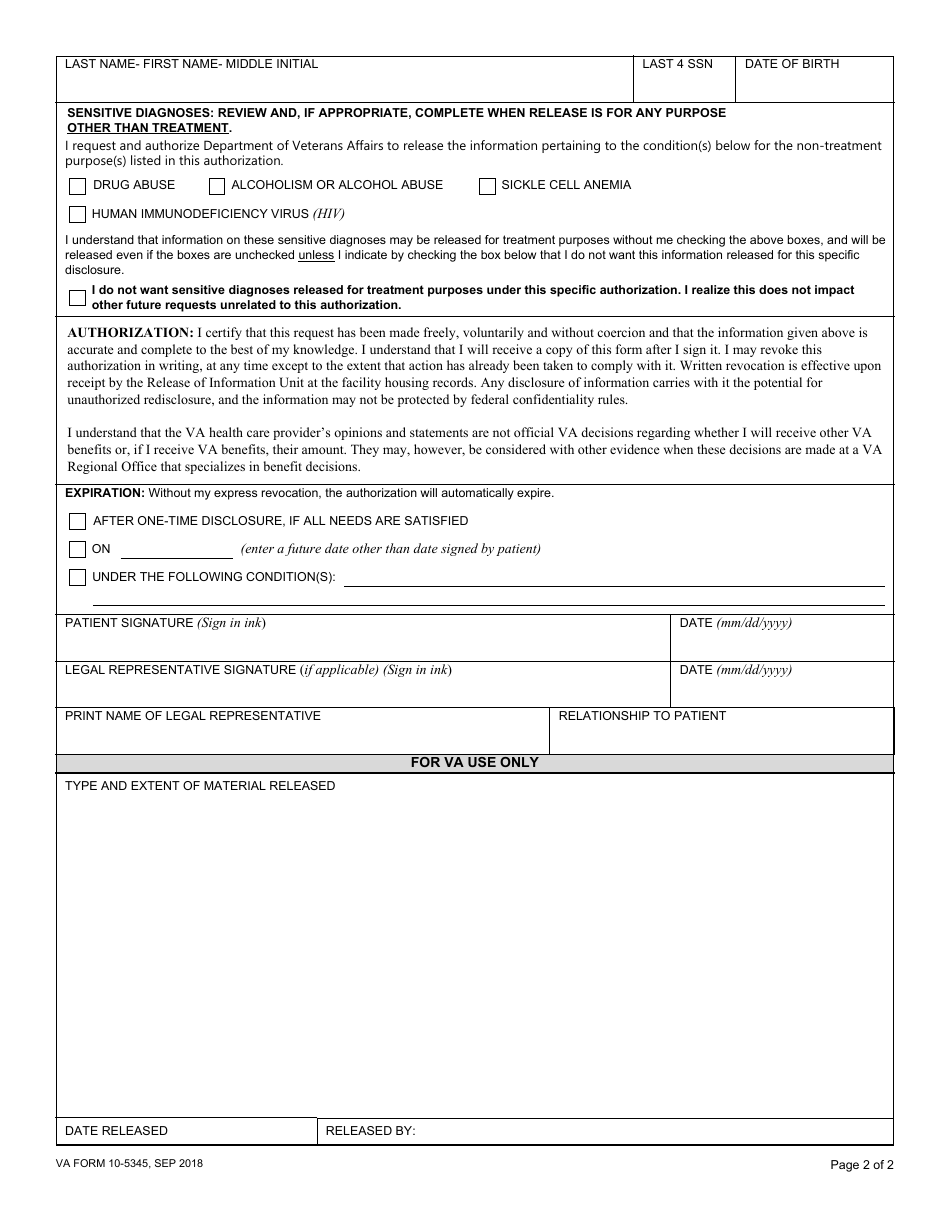
- If the medical data is released for non-treatment purposes, review and complete the "Sensitive Diagnoses" section. The information on the diagnoses mentioned in this section will be disclosed for treatment purposes without your consent. If you do not wish the information to be disclosed, to check the box below that states your refusal to release this specific information.
- Read the authorization statement carefully.
- Select the authorization expiration date or conditions in the "Expiration" section.
- Sign and date the form. The paper can be signed by your legal representative.
The bottom of the form is reserved for VA use only.
Where to Send VA Form 10-5345?
The completed and signed VA 10-5345 should be sent to the specific VA health care facility where the veteran was treated. In case you need to release medical information concerning the treatment in several different VA healthcare facilities, you are required to submit a separate form to each of them.
Download VA Form 10-5345 Request for and Authorization to Release Health Information
1
2