![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form FA-92
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form FA-92
for the current year.
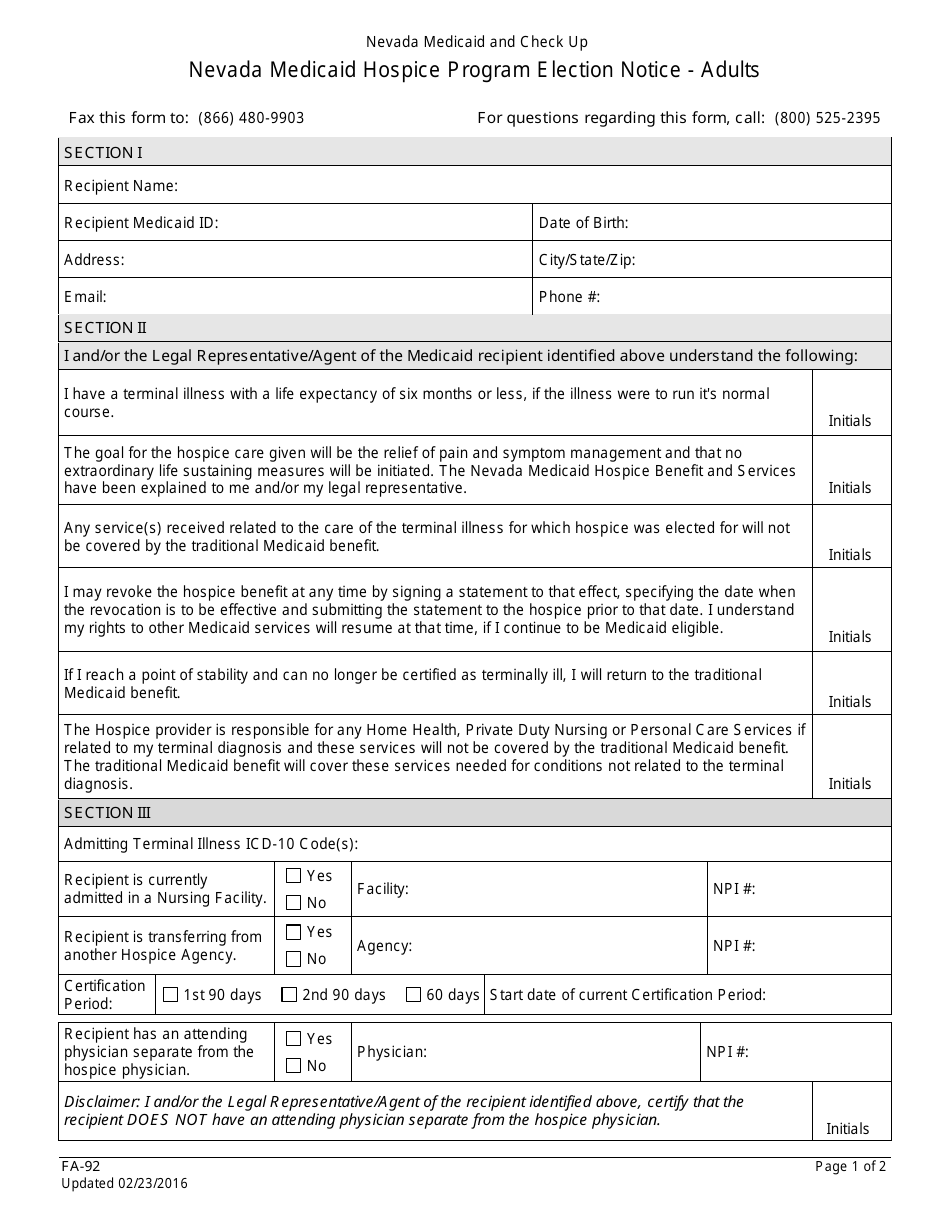
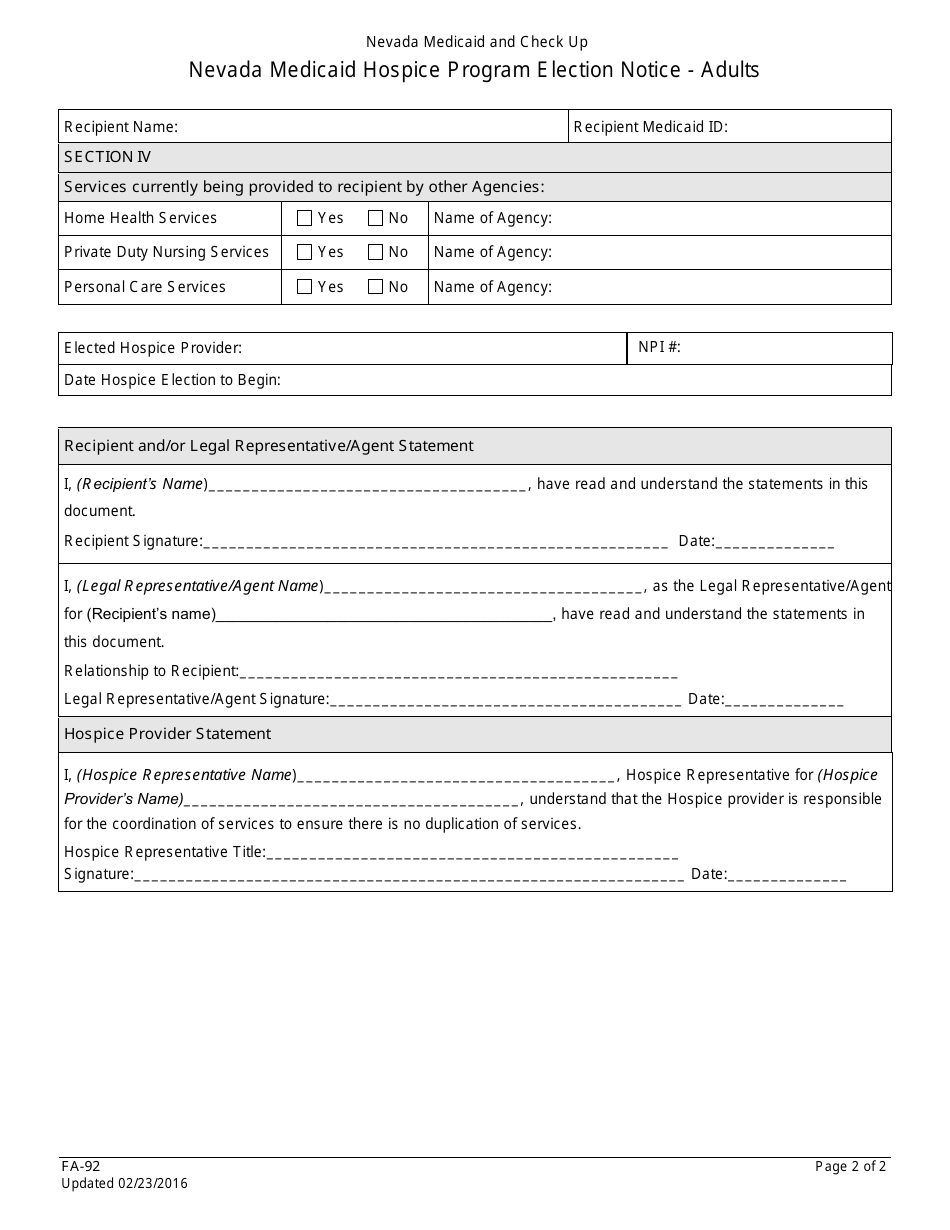
Form FA-92 Nevada Medicaid Hospice Program Election Notice - Adults - Nevada
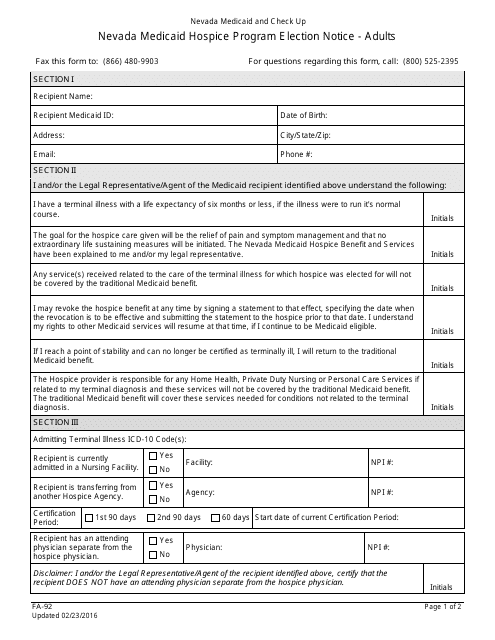
What Is Form FA-92?
This is a legal form that was released by the Nevada Department of Health and Human Services - a government authority operating within Nevada. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form FA-92?
A: Form FA-92 is a Nevada Medicaid Hospice Program Election Notice for adults.
Q: Who is this form for?
A: This form is for adults who are eligible for the Nevada Medicaid Hospice Program.
Q: What is the purpose of this form?
A: The purpose of this form is to notify the Medicaid program of the individual's election to receive hospice care.
Q: How do I fill out Form FA-92?
A: You will need to provide your personal information, such as your name, address, and Medicaid ID number. You will also need to indicate your choice to enroll in the Medicaid Hospice Program.
Q: Are there any eligibility requirements for the Medicaid Hospice Program?
A: Yes, you must meet certain criteria to be eligible for the Medicaid Hospice Program, including having a terminal illness and a life expectancy of no more than six months.
Q: What services are covered under the Medicaid Hospice Program?
A: The Medicaid Hospice Program covers a range of services, including medical care, pain relief, counseling, and support for both the individual and their family.
Q: Can I change my mind after electing to enroll in the Medicaid Hospice Program?
A: Yes, you can change your mind at any time and revoke your election to receive hospice care.
Q: What should I do if I have questions about Form FA-92 or the Medicaid Hospice Program?
A: If you have any questions or need more information, you should contact your Medicaid provider or the Nevada Medicaid office.
Form Details:
- Released on February 23, 2016;
- The latest edition provided by the Nevada Department of Health and Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form FA-92 by clicking the link below or browse more documents and templates provided by the Nevada Department of Health and Human Services.
Download Form FA-92 Nevada Medicaid Hospice Program Election Notice - Adults - Nevada
1
2