![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form DHS-3887-ENG
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form DHS-3887-ENG
for the current year.
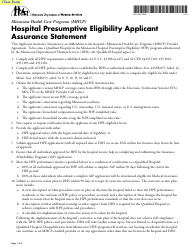
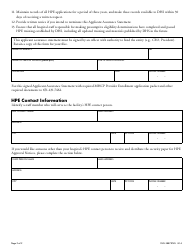
Form DHS-3887-ENG Hospital Presumptive Eligibility Applicant Assurance Statement - Minnesota
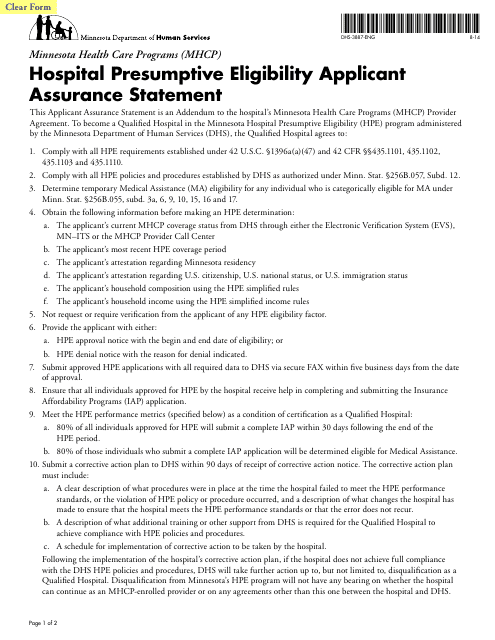
What Is Form DHS-3887-ENG?
This is a legal form that was released by the Minnesota Department of Human Services - a government authority operating within Minnesota. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is DHS-3887-ENG?
A: DHS-3887-ENG is a form for Hospital Presumptive Eligibility Applicant Assurance Statement.
Q: What is Hospital Presumptive Eligibility?
A: Hospital Presumptive Eligibility is a temporary Medicaid coverage for individuals who qualify based on their hospital stay or emergency medical condition.
Q: Who needs to complete the form?
A: Minnesota residents who are applying for Hospital Presumptive Eligibility need to complete the DHS-3887-ENG form.
Q: What does the form require?
A: The form requires applicants to provide their personal information, income, household size, and other relevant details.
Q: Is the form available in languages other than English?
A: Yes, the form is available in languages other than English, including Spanish and Somali.
Q: What is the purpose of the form?
A: The purpose of the form is to collect necessary information to determine an applicant's eligibility for Hospital Presumptive Eligibility.
Q: How long does the coverage last?
A: Hospital Presumptive Eligibility coverage lasts for 60 days.
Q: Can I apply for other Medicaid programs while on Hospital Presumptive Eligibility?
A: Yes, individuals can apply for other Medicaid programs while on Hospital Presumptive Eligibility.
Form Details:
- Released on August 1, 2014;
- The latest edition provided by the Minnesota Department of Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHS-3887-ENG by clicking the link below or browse more documents and templates provided by the Minnesota Department of Human Services.
Download Form DHS-3887-ENG Hospital Presumptive Eligibility Applicant Assurance Statement - Minnesota
1
2