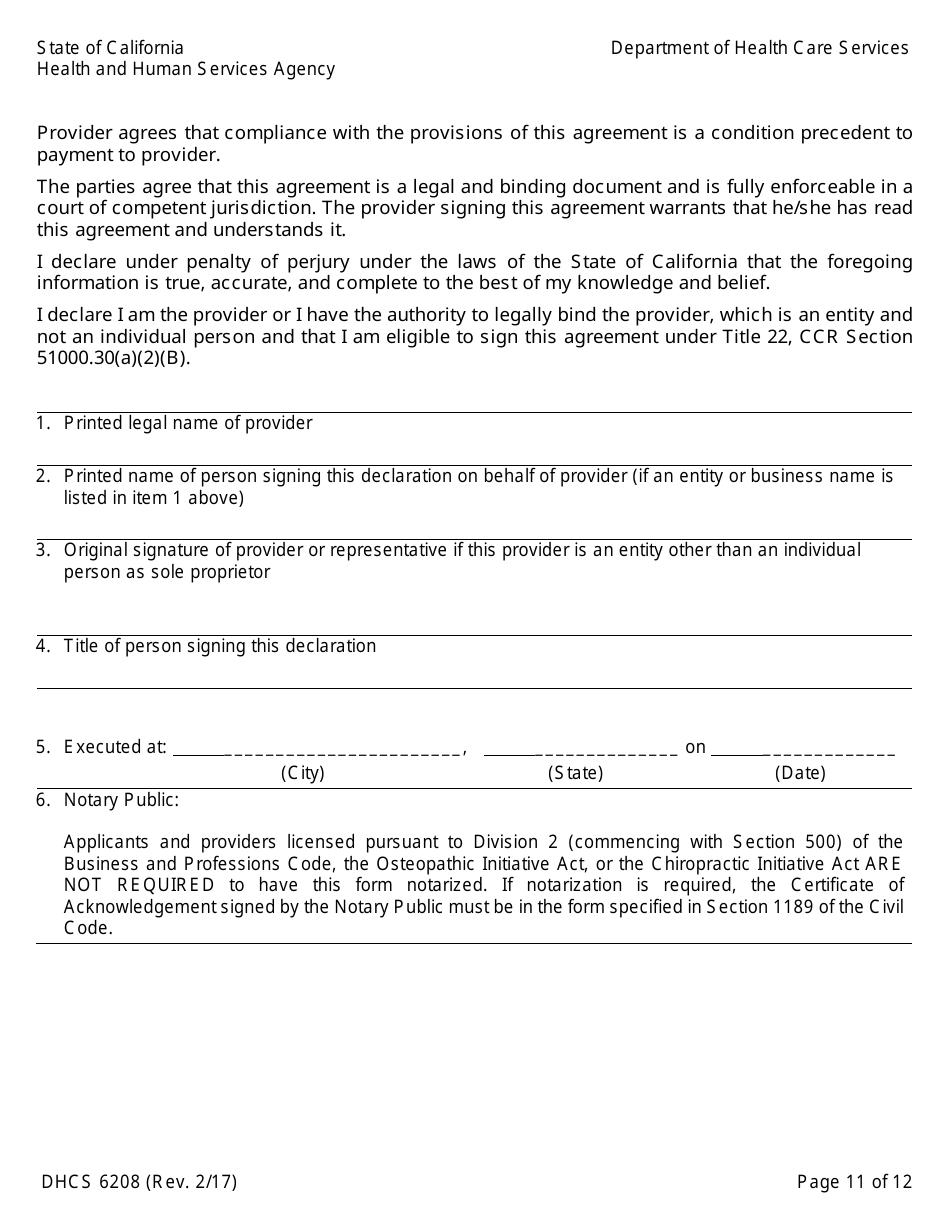
Form DHCS6208 Medi-Cal Provider Agreement (To Accompany Applications for Enrollment or Continued Enrollment) - California
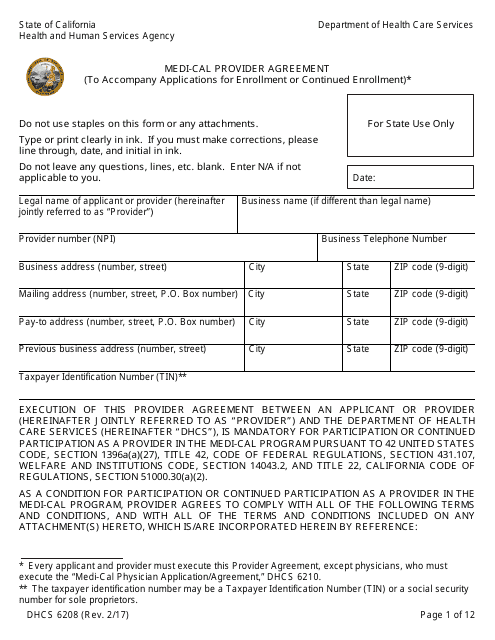
What Is Form DHCS6208?
This is a legal form that was released by the California Department of Health Care Services - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
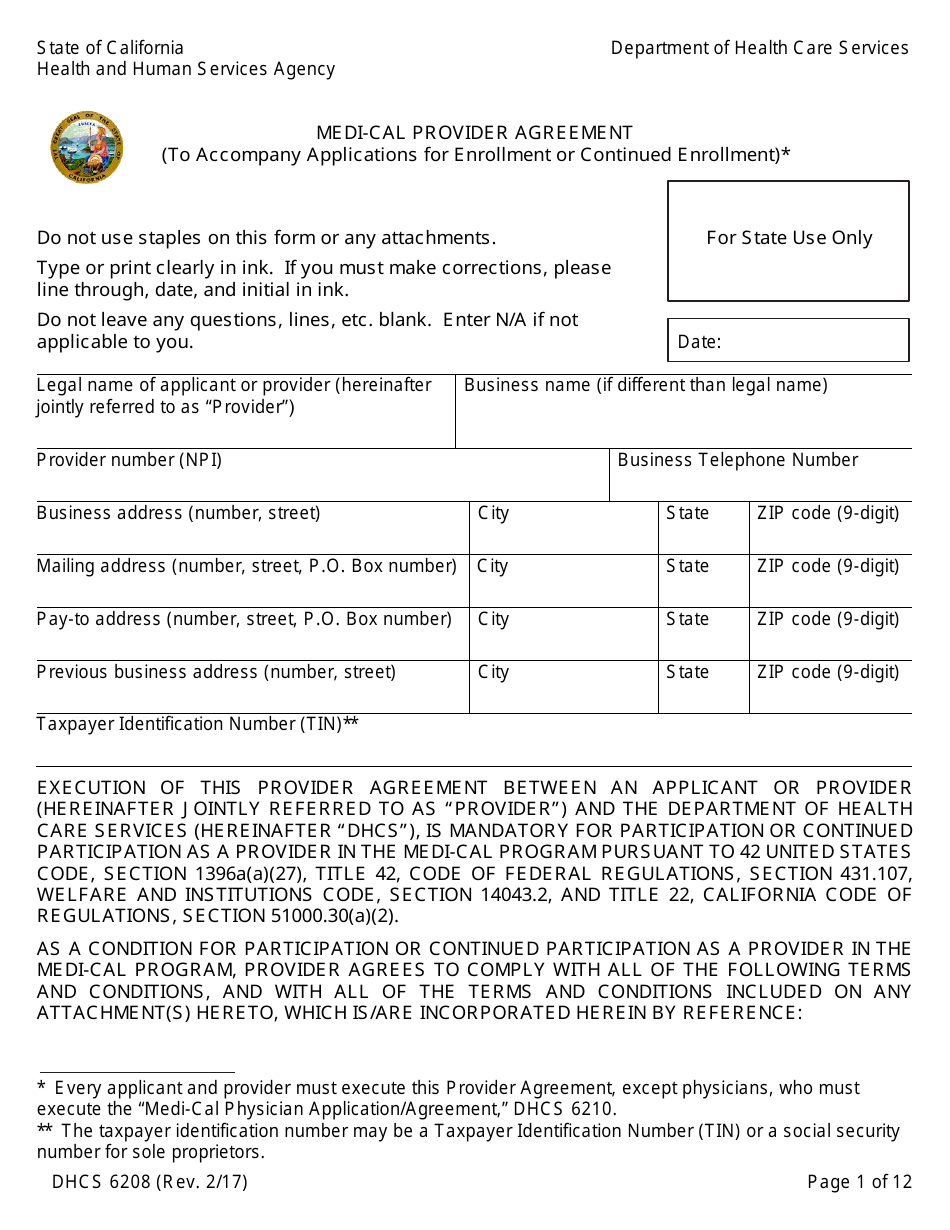
Q: What is the DHCS6208 form?
A: The DHCS6208 form is the Medi-Cal Provider Agreement to accompany applications for enrollment or continued enrollment.
Q: What is Medi-Cal?
A: Medi-Cal is California's Medicaid program that provides free or low-cost health coverage to low-income individuals and families.
Q: Who needs to complete the DHCS6208 form?
A: Providers who wish to enroll or continue their enrollment in the Medi-Cal program need to complete the DHCS6208 form.
Q: What information is required on the DHCS6208 form?
A: The DHCS6208 form requires providers to provide their personal information, business details, and agree to the terms and conditions of the Medi-Cal program.
Q: How often does the DHCS6208 form need to be completed?
A: The DHCS6208 form needs to be completed when initially applying for enrollment in the Medi-Cal program and may need to be updated annually or when there are changes to the provider's information.
Q: What is the purpose of the DHCS6208 form?
A: The purpose of the DHCS6208 form is to collect necessary information from providers and ensure they agree to the terms and conditions of participation in the Medi-Cal program.
Q: Are there any fees associated with the DHCS6208 form?
A: There are no fees associated with completing and submitting the DHCS6208 form.
Q: What happens after submitting the DHCS6208 form?
A: After submitting the DHCS6208 form, the provider's application for enrollment or continued enrollment in the Medi-Cal program will be reviewed by the California Department of Health Care Services.
Form Details:
- Released on February 1, 2017;
- The latest edition provided by the California Department of Health Care Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHCS6208 by clicking the link below or browse more documents and templates provided by the California Department of Health Care Services.
Download Form DHCS6208 Medi-Cal Provider Agreement (To Accompany Applications for Enrollment or Continued Enrollment) - California
1

2

3

4

5

6
7

8
9
10
11

12