Form DHCS4029 Medi-Cal Rendering Provider / Group Affiliation / Disaffiliation Form - California
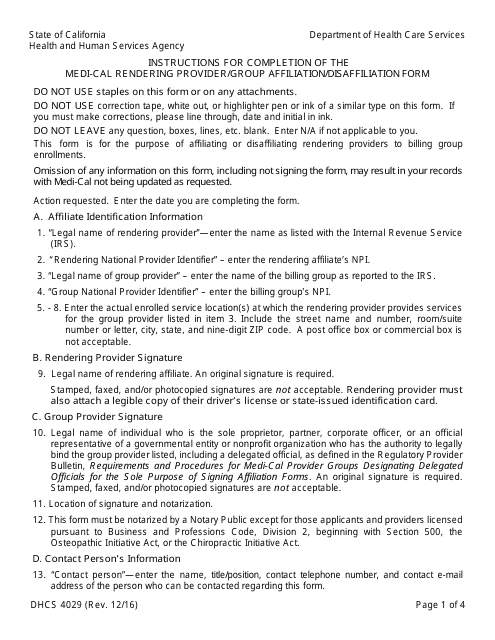
What Is Form DHCS4029?
This is a legal form that was released by the California Department of Health Care Services - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is DHCS4029 form?
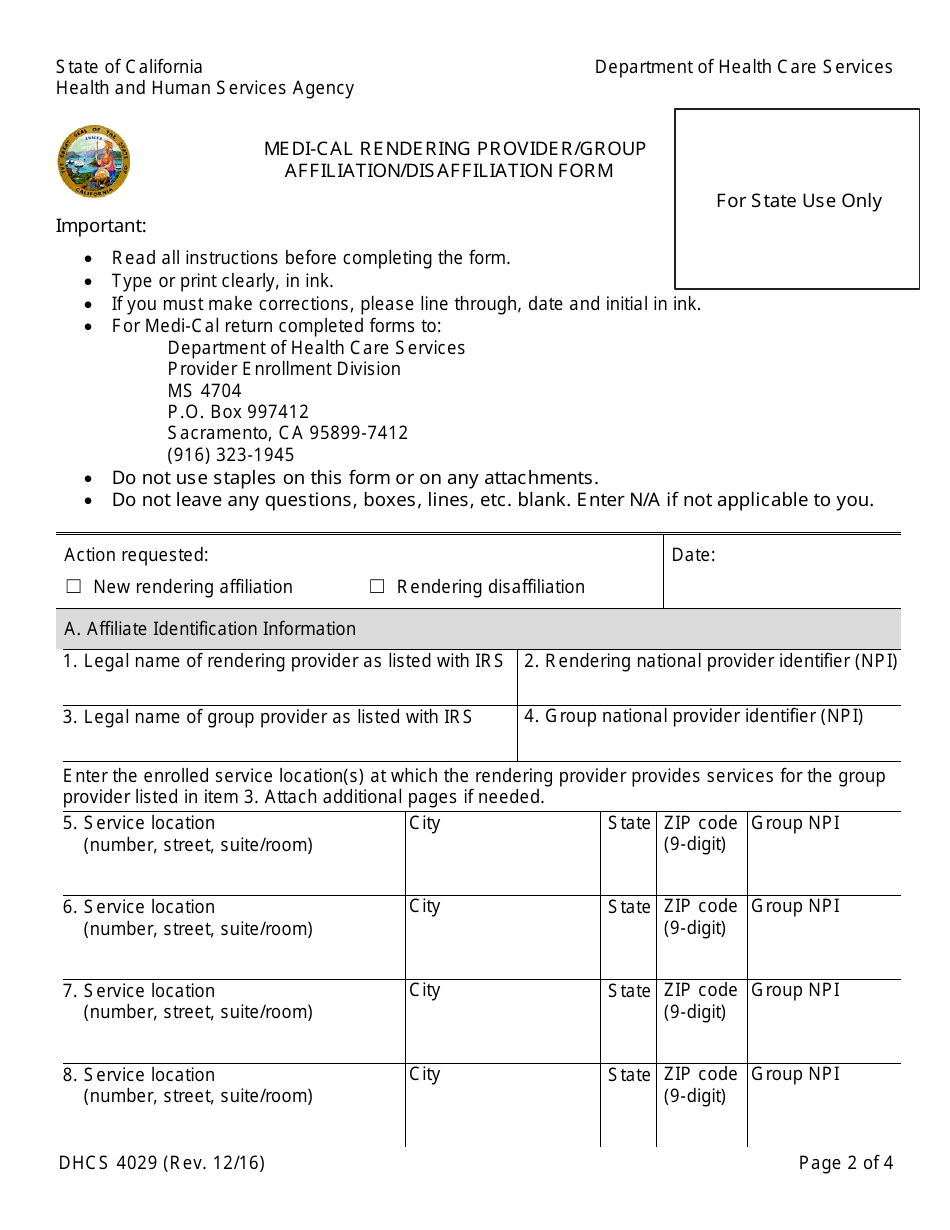
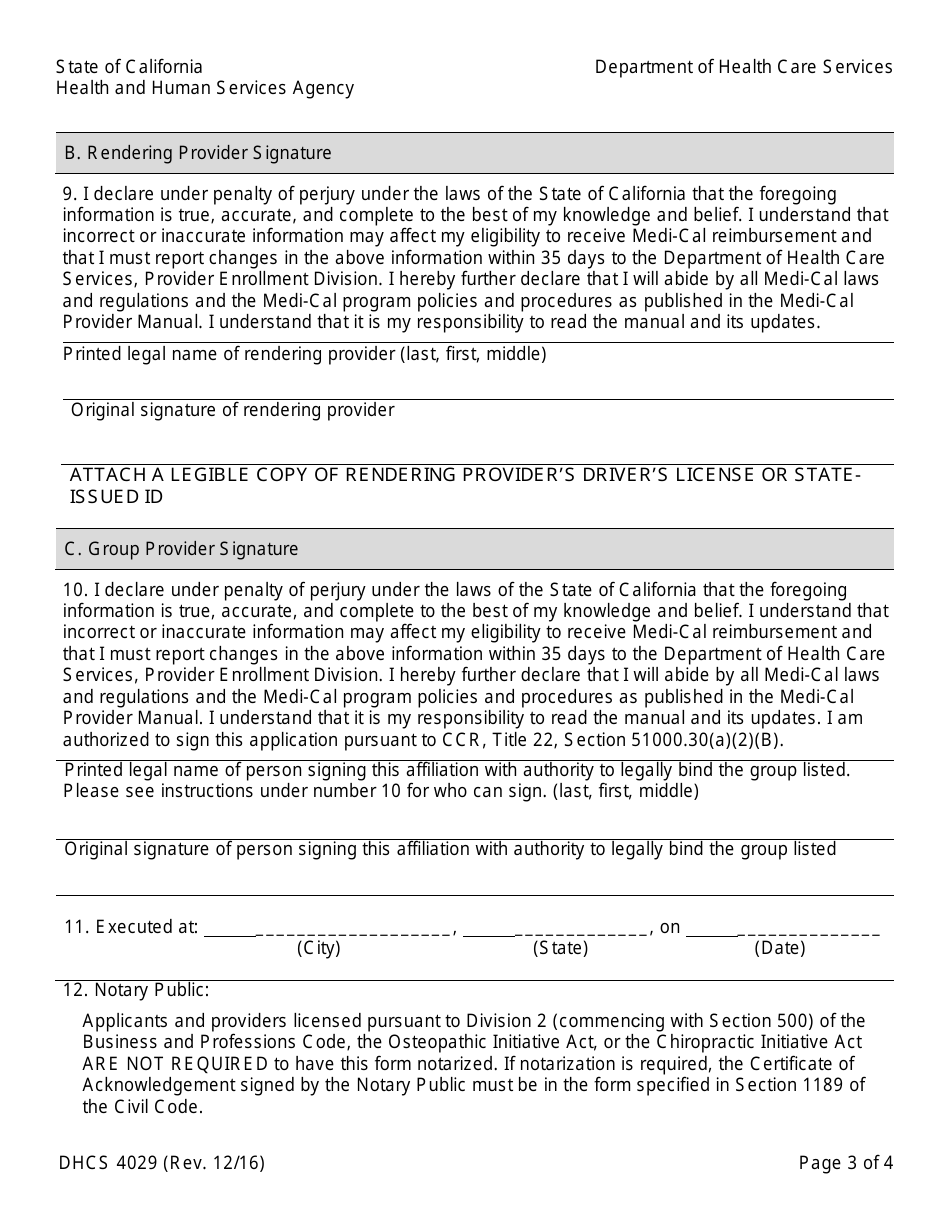
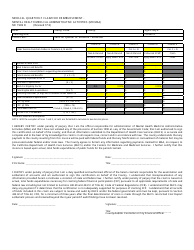
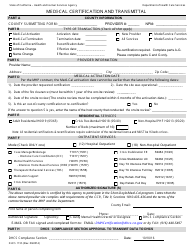
A: DHCS4029 form is the Medi-Cal Rendering Provider/Group Affiliation/Disaffiliation Form used in California.
Q: What is the purpose of DHCS4029 form?
A: The purpose of DHCS4029 form is to request affiliation or disaffiliation of a rendering provider or group with a Medi-Cal provider or group.
Q: Who needs to use DHCS4029 form?
A: DHCS4029 form needs to be used by rendering providers or groups who want to affiliate or disaffiliate with a Medi-Cal provider or group.
Q: Are there any fees associated with DHCS4029 form?
A: There are no fees associated with submitting the DHCS4029 form.
Q: How should I submit the DHCS4029 form?
A: The DHCS4029 form should be submitted electronically through the Medi-Cal Provider Enrollment Portal or by mail to the address provided on the form.
Q: Is the DHCS4029 form required for all providers?
A: No, the DHCS4029 form is only required for rendering providers or groups affiliating or disaffiliating with a Medi-Cal provider or group.
Form Details:
- Released on December 1, 2016;
- The latest edition provided by the California Department of Health Care Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHCS4029 by clicking the link below or browse more documents and templates provided by the California Department of Health Care Services.
Download Form DHCS4029 Medi-Cal Rendering Provider / Group Affiliation / Disaffiliation Form - California
1
2

3

4