Form DHCS100185 Drug Medi-Cal (Dmc) Claim Submission Certification - Direct Contract Provider - California
What Is Form DHCS100185?
This is a legal form that was released by the California Department of Health Care Services - a government authority operating within California. Check the official instructions before completing and submitting the form.
FAQ
Q: What is DHCS100185?
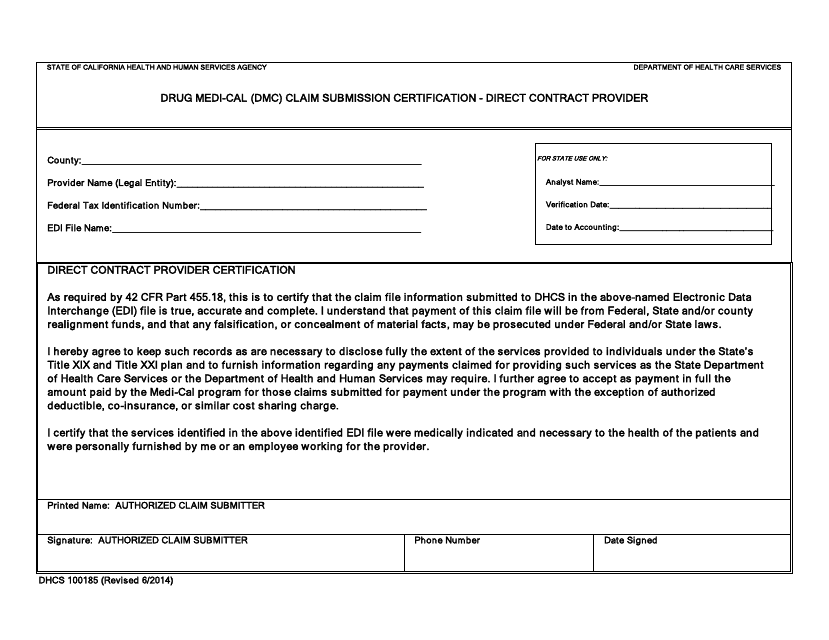
A: DHCS100185 is a form used for Drug Medi-Cal (DMC) Claim Submission Certification for Direct Contract Providers in California.
Q: Who is required to submit DHCS100185?
A: Direct Contract Providers participating in the Drug Medi-Cal (DMC) program in California are required to submit DHCS100185.
Q: What is the purpose of DHCS100185?
A: The purpose of DHCS100185 is to certify that the Direct Contract Provider is in compliance with certain requirements for claiming reimbursement under the Drug Medi-Cal (DMC) program.
Q: What information is required on DHCS100185?
A: DHCS100185 requires information such as the provider's name, address, contract number, and certification of compliance with DMC program requirements.
Q: Are there any deadlines for submitting DHCS100185?
A: Yes, Direct Contract Providers must submit DHCS100185 within 120 days of the effective date of the contract or within 30 days of receipt of the form.
Q: Can DHCS100185 be submitted electronically?
A: Yes, DHCS100185 can be submitted electronically through the provider's designated Drug Medi-Cal (DMC) portal.
Q: Is DHCS100185 a one-time submission?
A: No, DHCS100185 must be submitted annually by Direct Contract Providers participating in the Drug Medi-Cal (DMC) program.
Q: What happens if DHCS100185 is not submitted?
A: Failure to submit DHCS100185 may result in denial of reimbursement for services provided under the Drug Medi-Cal (DMC) program.
Q: Are there any additional requirements for Direct Contract Providers under the Drug Medi-Cal (DMC) program?
A: Yes, Direct Contract Providers must also comply with other program requirements such as maintaining required licensure and certifications, providing medically necessary services, and maintaining documentation for audits and reviews.
Form Details:
- Released on June 1, 2014;
- The latest edition provided by the California Department of Health Care Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHCS100185 by clicking the link below or browse more documents and templates provided by the California Department of Health Care Services.