Form DMHC20-224 Imr Application / Complaint Form - California (Korean)
This is a legal form that was released by the California Department of Managed Health Care - a government authority operating within California.
The document is provided in Korean. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
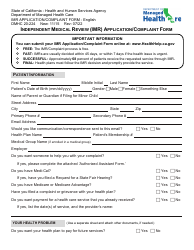
Q: What is the DMHC20-224 Imr Application/Complaint Form?
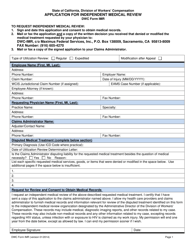
A: The DMHC20-224 Imr Application/Complaint Form is a form used in California for filing an application or complaint related to medical coverage.
Q: Who can use the DMHC20-224 Imr Application/Complaint Form?
A: Any person who is seeking to appeal a decision made by a health plan or has a complaint related to their medical coverage in California can use this form.
Q: What is the purpose of the DMHC20-224 Imr Application/Complaint Form?
A: The purpose of this form is to request an independent medical review (IMR) or file a complaint with the California Department of Managed Health Care (DMHC) regarding medical coverage issues.
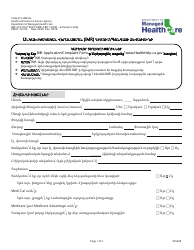
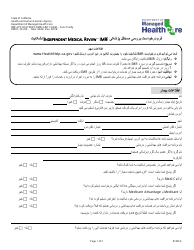
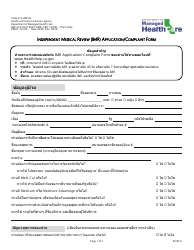
Q: Is the DMHC20-224 Imr Application/Complaint Form available in Korean?
A: Yes, the DMHC20-224 Imr Application/Complaint Form is available in Korean for those who prefer to fill it out in that language.
Q: Is there a fee for submitting the DMHC20-224 Imr Application/Complaint Form?
A: No, there is no fee for submitting the DMHC20-224 Imr Application/Complaint Form.
Q: What should I do after submitting the DMHC20-224 Imr Application/Complaint Form?
A: After submitting the form, you should receive a confirmation from the California Department of Managed Health Care (DMHC) acknowledging the receipt of your application or complaint. They will then process your request accordingly.
Form Details:
- Released on August 1, 2018;
- The latest edition provided by the California Department of Managed Health Care;
- Easy to use and ready to print;
- Available in Spanish;
- Quick to customize;
- Compatible with most PDF-viewing applications;
Download a printable version of Form DMHC20-224 by clicking the link below or browse more documents and templates provided by the California Department of Managed Health Care.
Download Form DMHC20-224 Imr Application / Complaint Form - California (Korean)
1
2
3
4
5
6

7