Form DHCS6065B Good Cause Certification - California
What Is Form DHCS6065B?
This is a legal form that was released by the California Department of Health Care Services - a government authority operating within California. Check the official instructions before completing and submitting the form.
FAQ
Q: What is Form DHCS6065B?
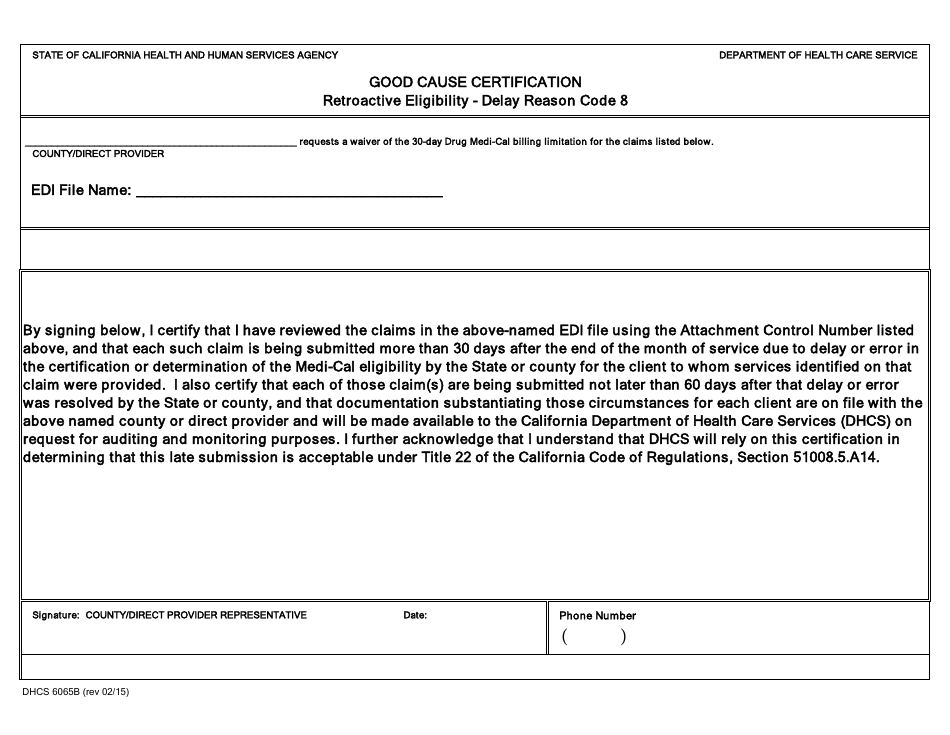
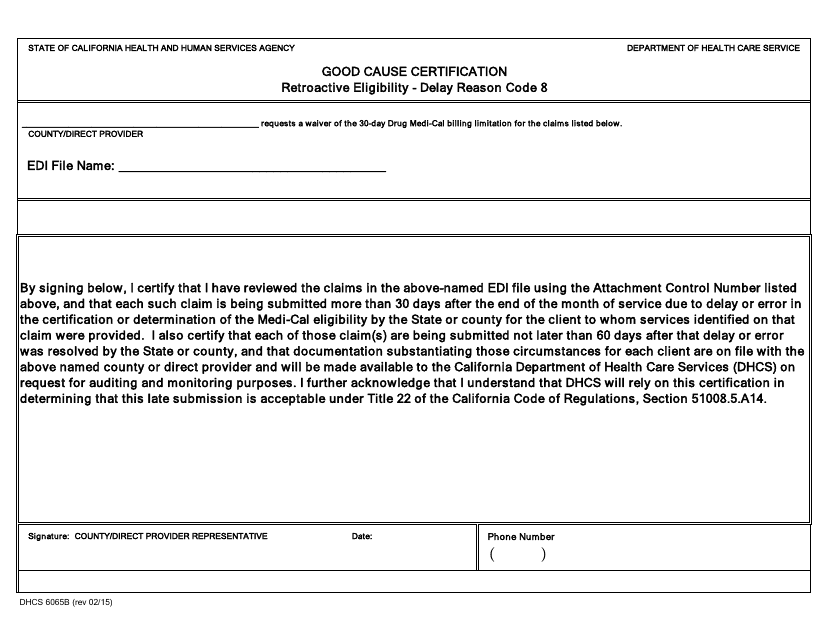
A: Form DHCS6065B is a Good Cause Certification form used in California.
Q: What is the purpose of Form DHCS6065B?
A: The purpose of Form DHCS6065B is to certify that an individual has a good cause for not meeting certain requirements for Medi-Cal eligibility.
Q: Who needs to fill out Form DHCS6065B?
A: Form DHCS6065B needs to be filled out by individuals applying for Medi-Cal who have a good cause for not meeting the eligibility requirements.
Q: What information is required on Form DHCS6065B?
A: Form DHCS6065B requires personal information of the applicant, details of the good cause, and supporting documentation if available.
Q: How should Form DHCS6065B be submitted?
A: Form DHCS6065B should be submitted to the local county Medi-Cal office.
Q: Can I request assistance in filling out Form DHCS6065B?
A: Yes, assistance can be requested from the county Medi-Cal office or other authorized individuals/agencies.
Q: Is there a deadline for submitting Form DHCS6065B?
A: The deadline for submitting Form DHCS6065B is usually within a specified time frame after the initial Medi-Cal application.
Q: What happens after submitting Form DHCS6065B?
A: After submitting Form DHCS6065B, the county Medi-Cal office will review the application and the good cause certification to determine eligibility.
Q: What if my Form DHCS6065B is denied?
A: If Form DHCS6065B is denied, the applicant has the right to request a hearing to appeal the decision.
Form Details:
- Released on February 1, 2015;
- The latest edition provided by the California Department of Health Care Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHCS6065B by clicking the link below or browse more documents and templates provided by the California Department of Health Care Services.