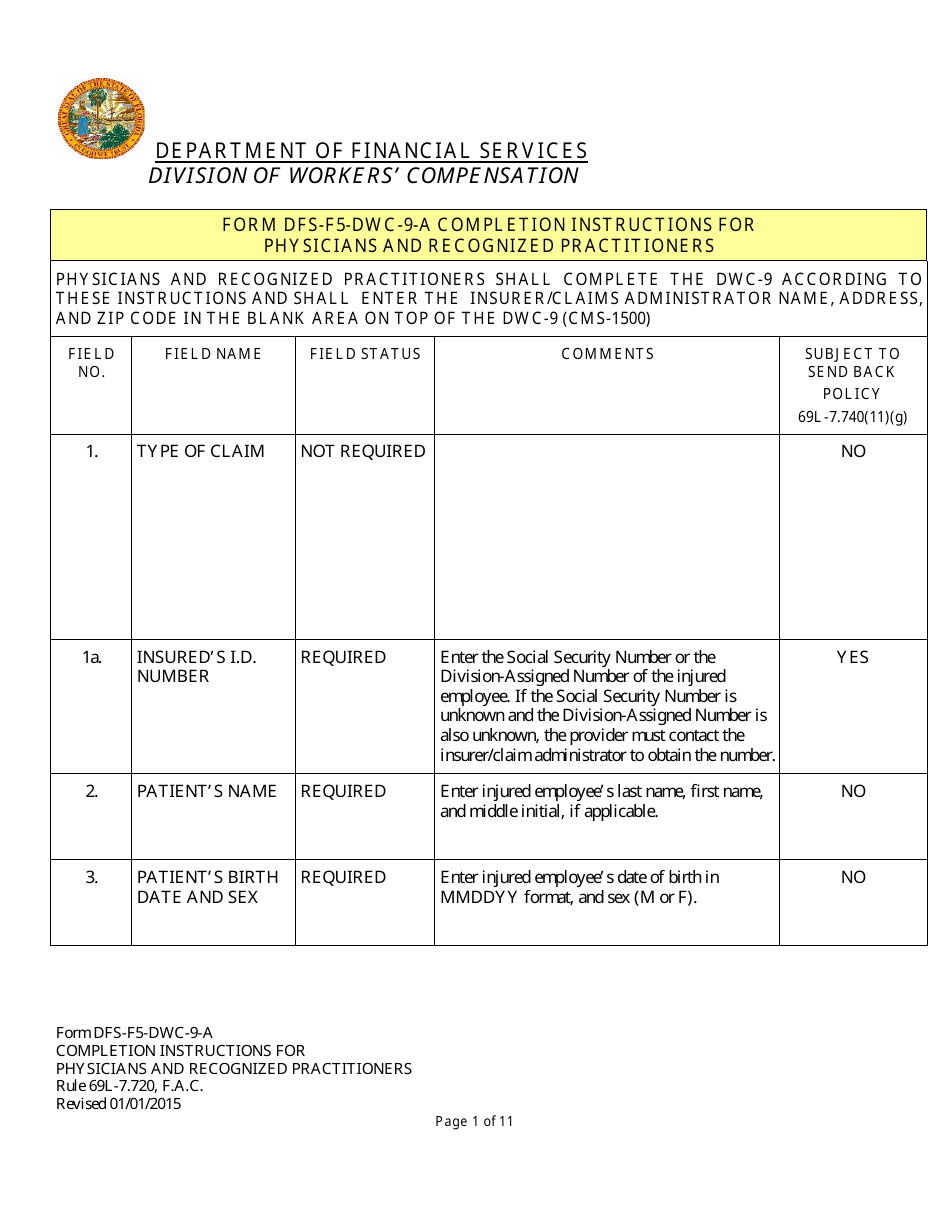
Instructions for Form DFS-F5-DWC-9 Health Insurance Claim Form (Licensed Health Care Providers) - Florida
This document contains official instructions for Form DFS-F5-DWC-9 , Health Insurance Claim Form (Licensed Health Care Providers) - a form released and collected by the Florida Department of Financial Services.
FAQ
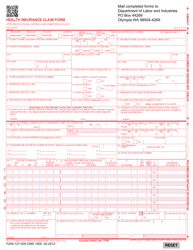
Q: What is Form DFS-F5-DWC-9?
A: Form DFS-F5-DWC-9 is a Health Insurance Claim Form for Licensed Health Care Providers in Florida.
Q: Who is this form for?
A: This form is for licensed health care providers in Florida who need to submit a health insurance claim.
Q: What is the purpose of this form?
A: The purpose of this form is to provide information about the health care services provided and to request payment from the health insurance company.
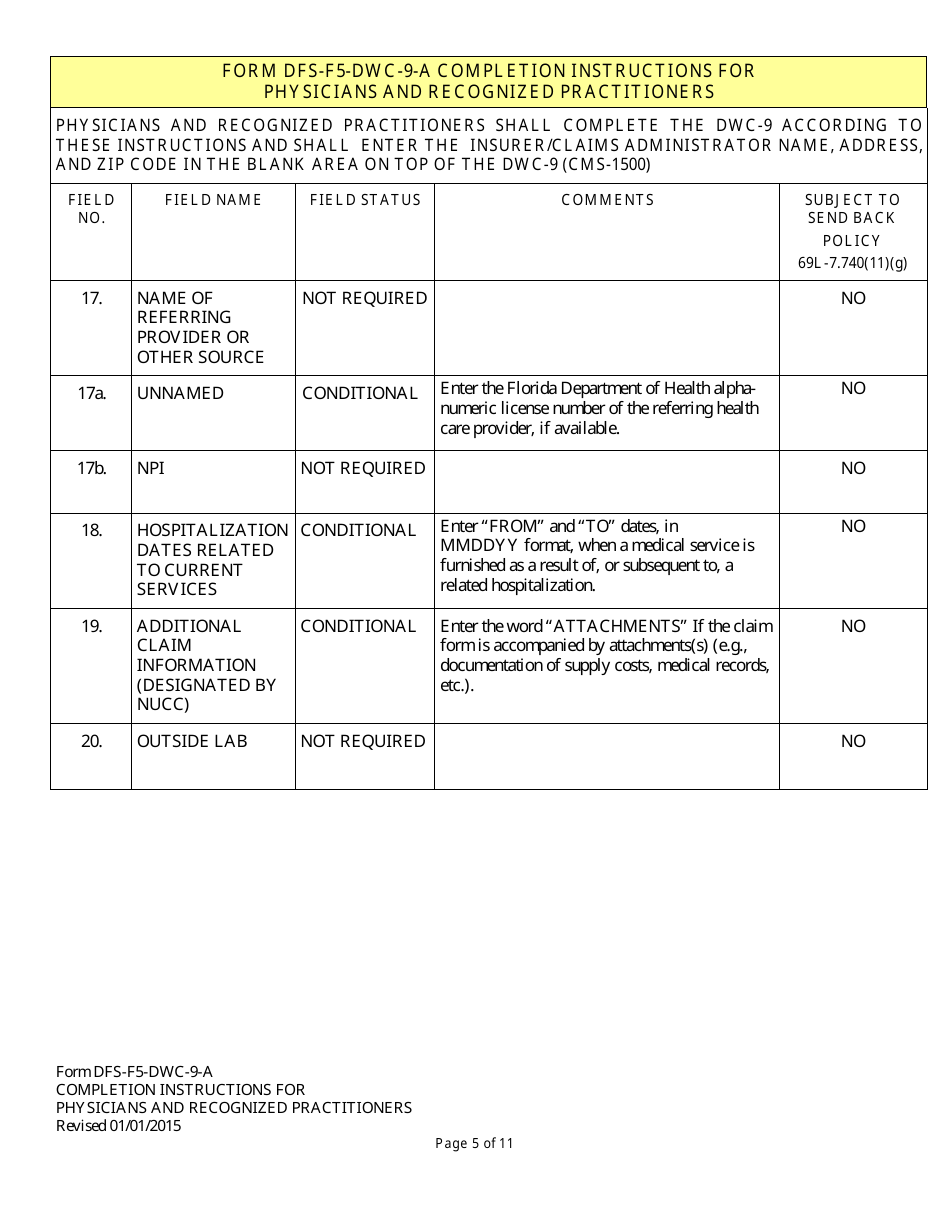
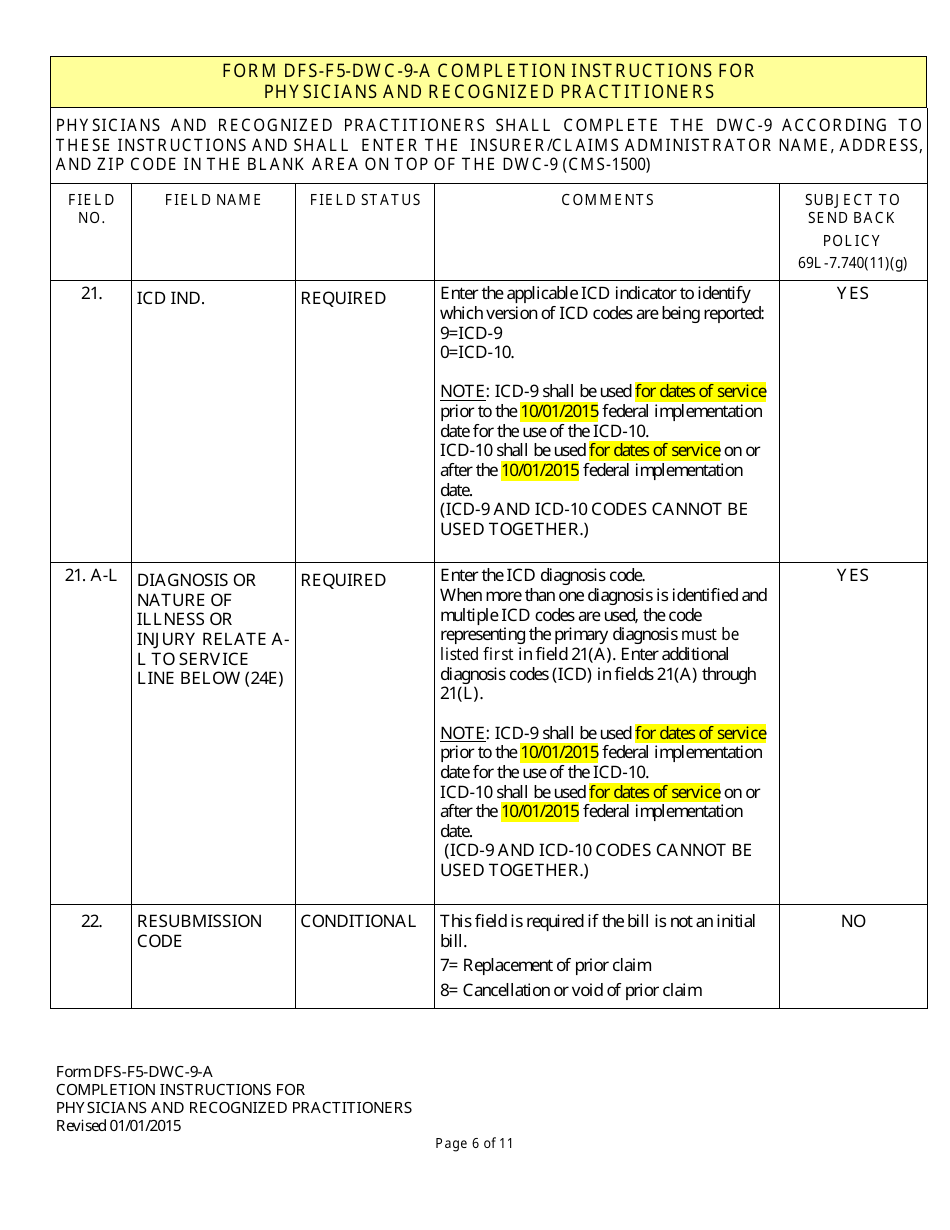
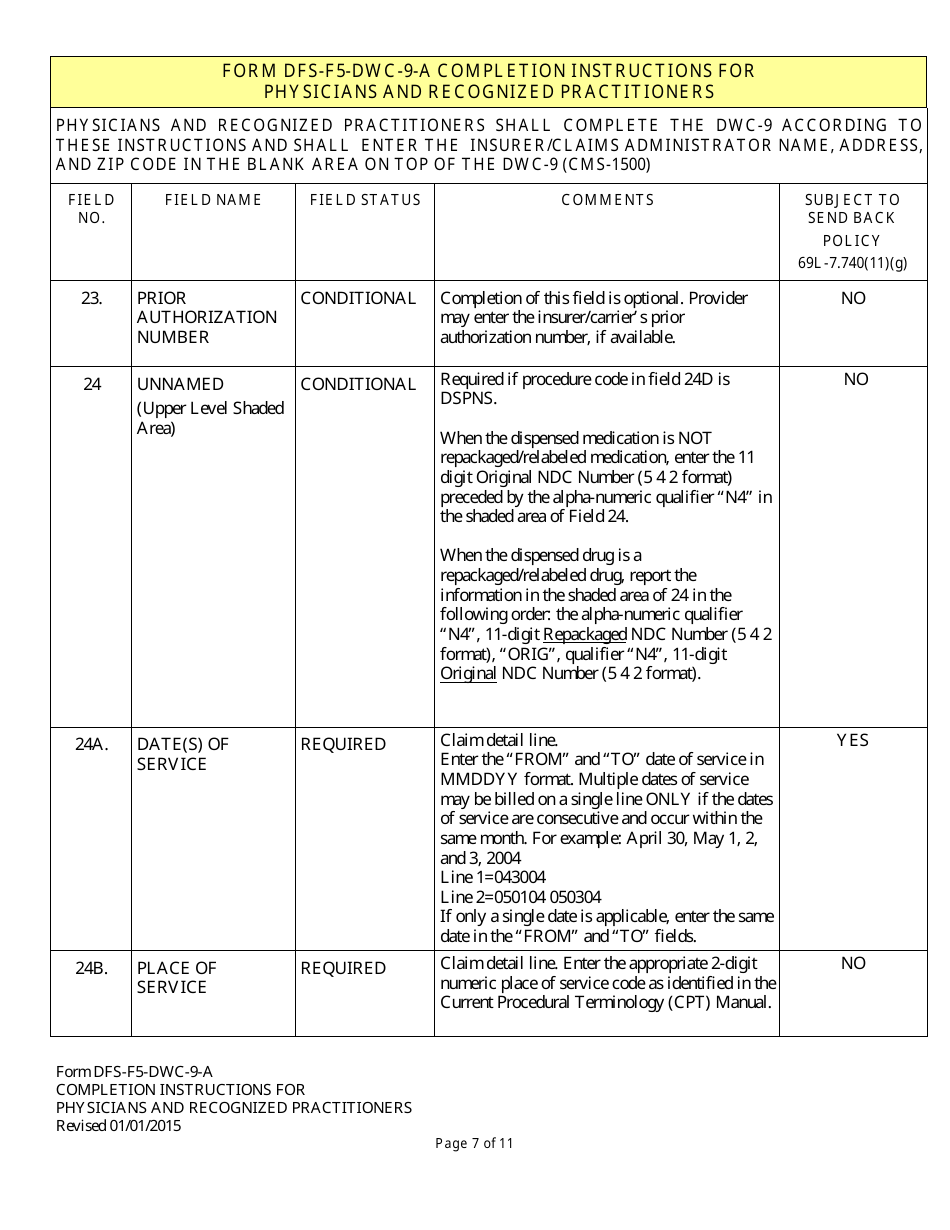
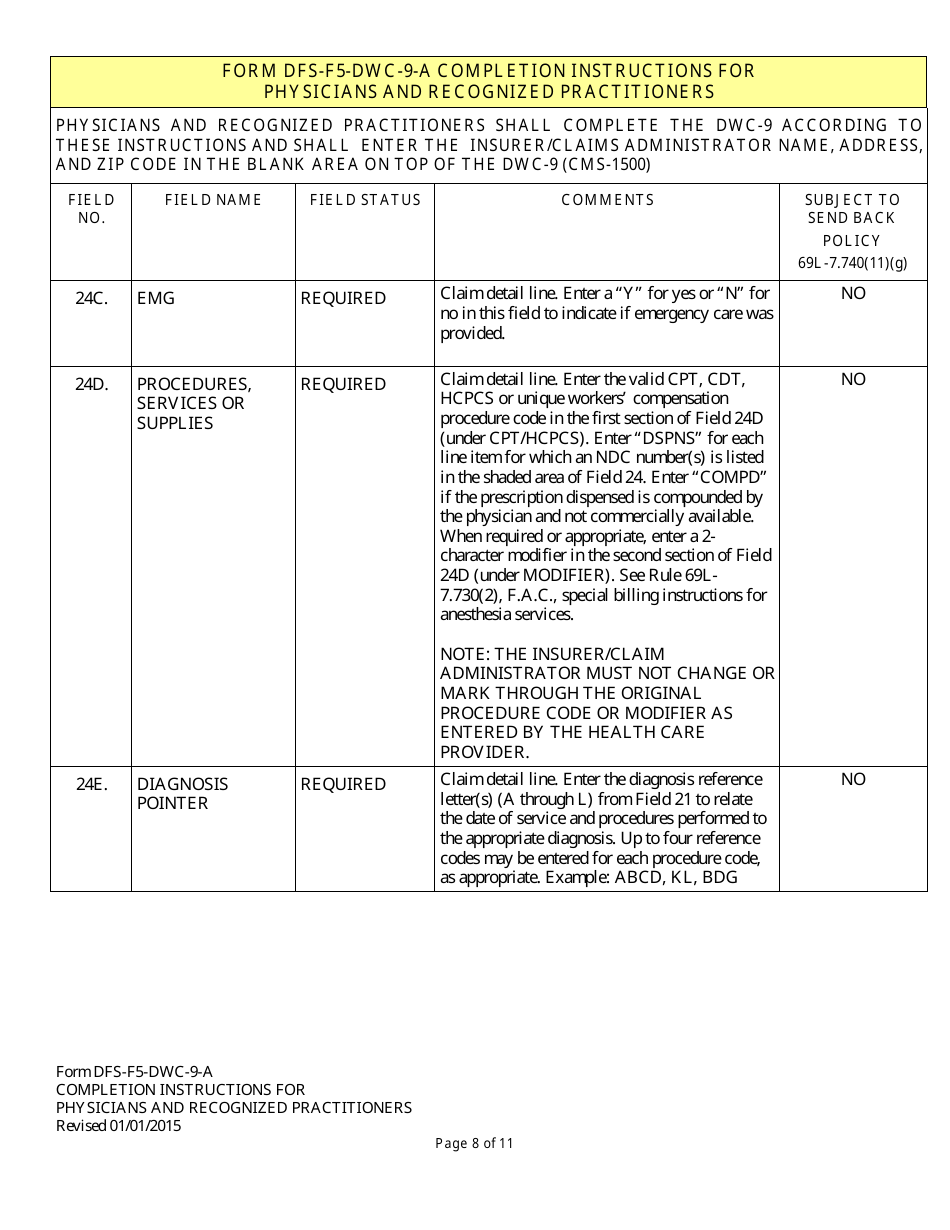
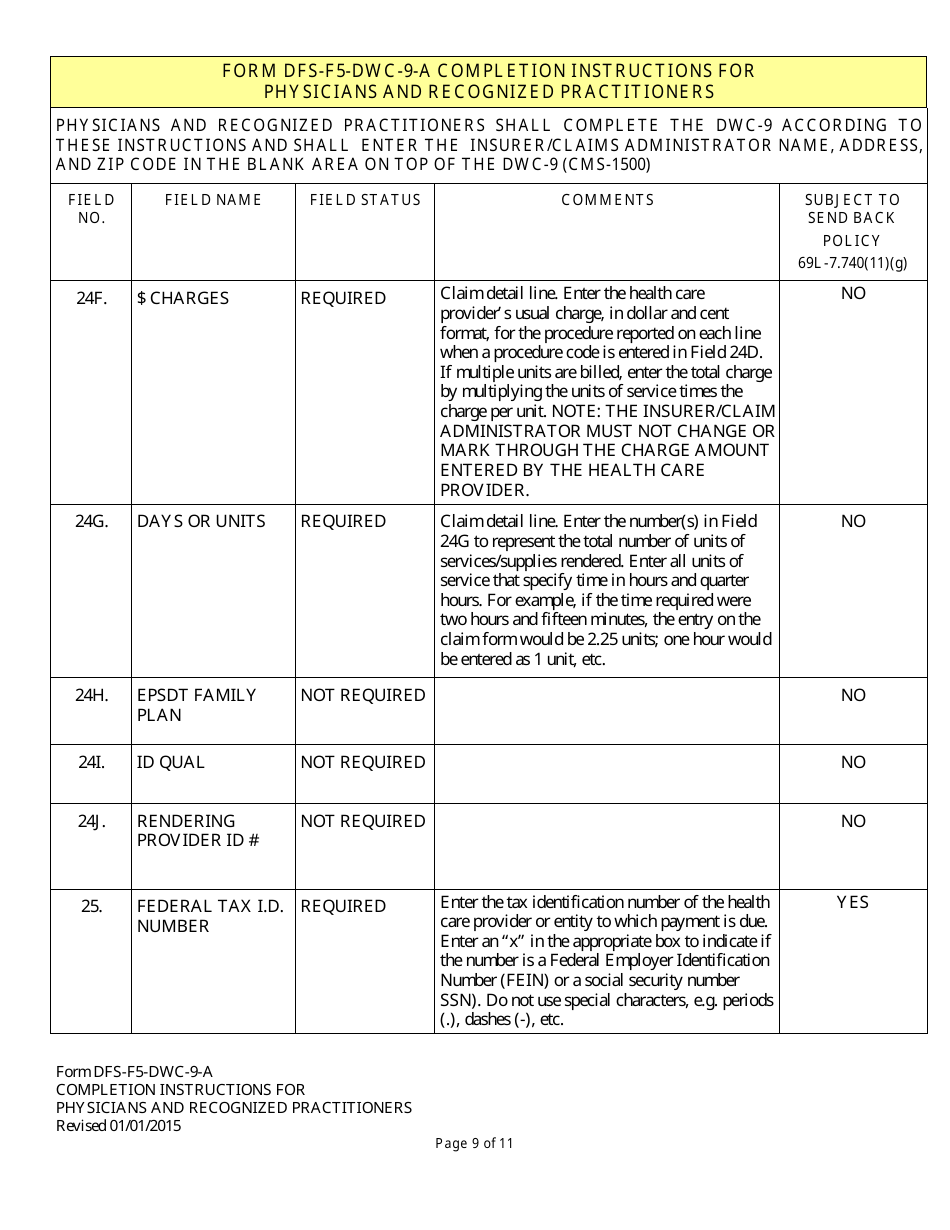
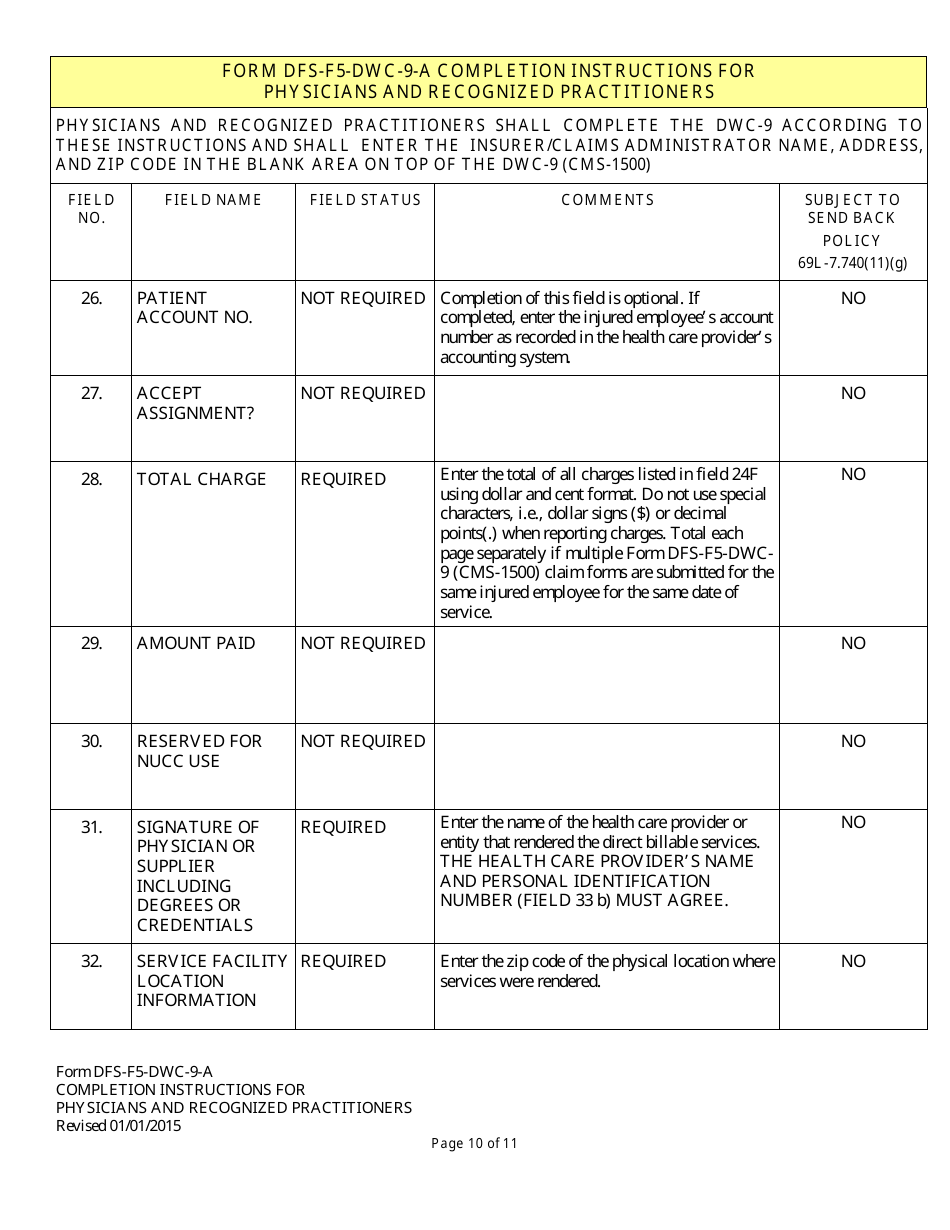
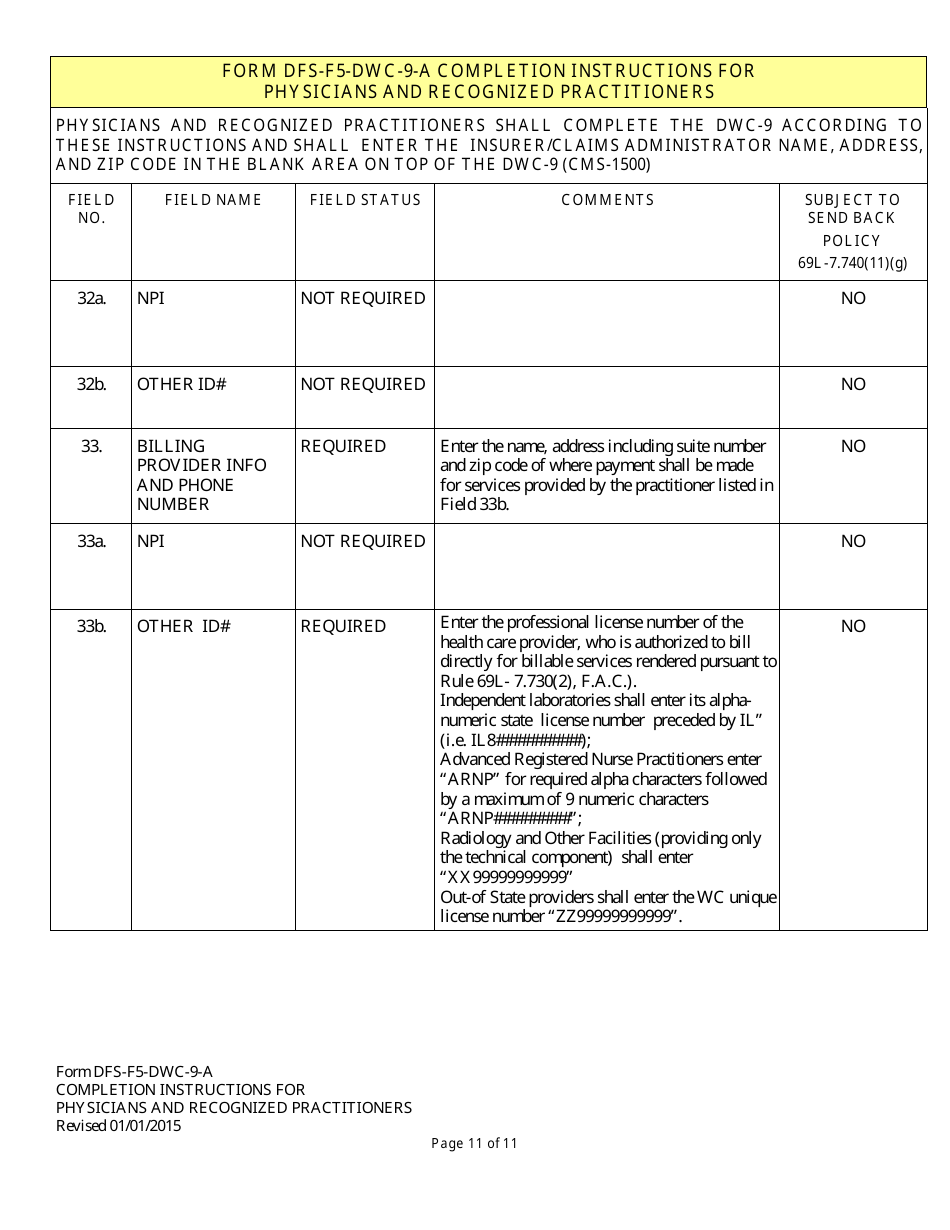
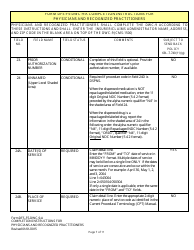
Q: What information is required on this form?
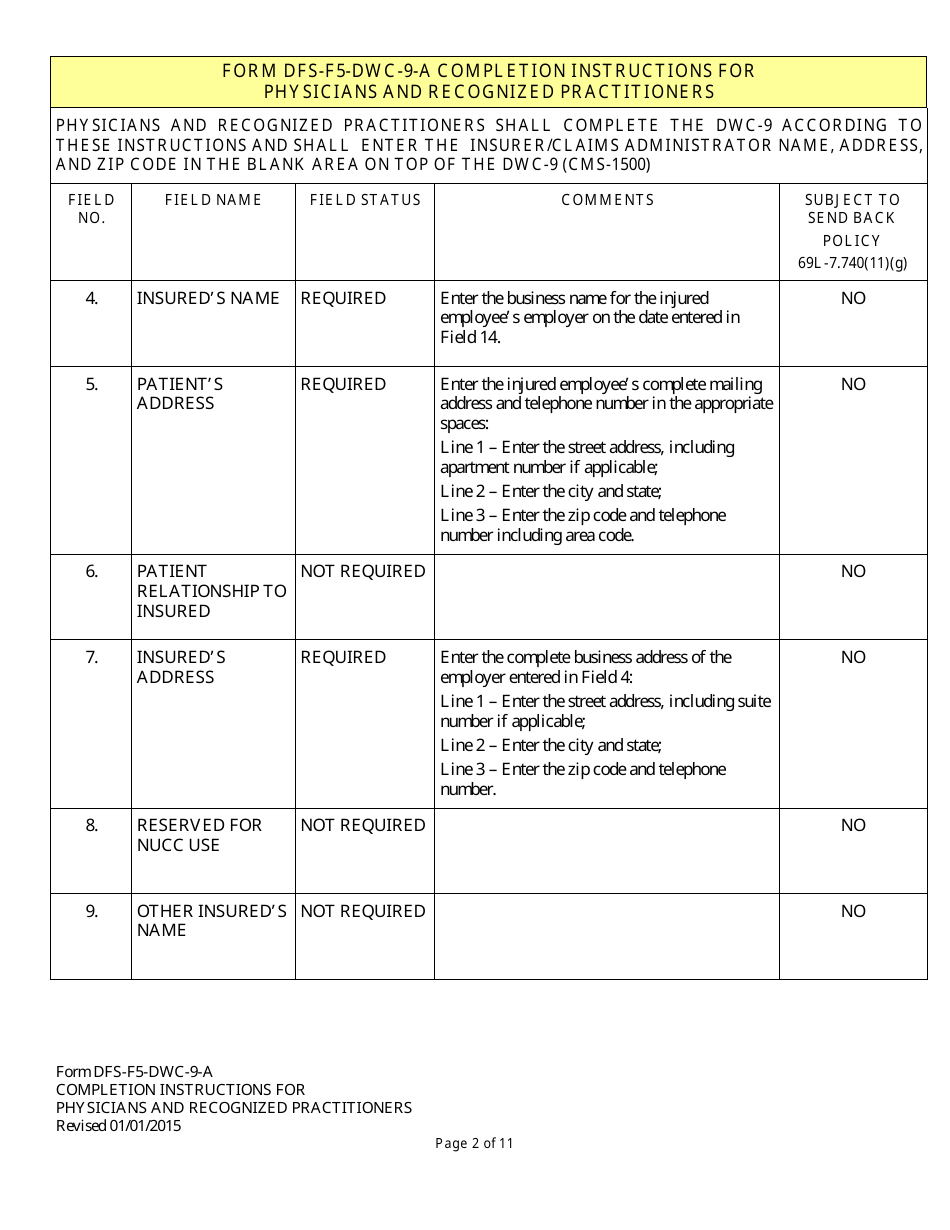
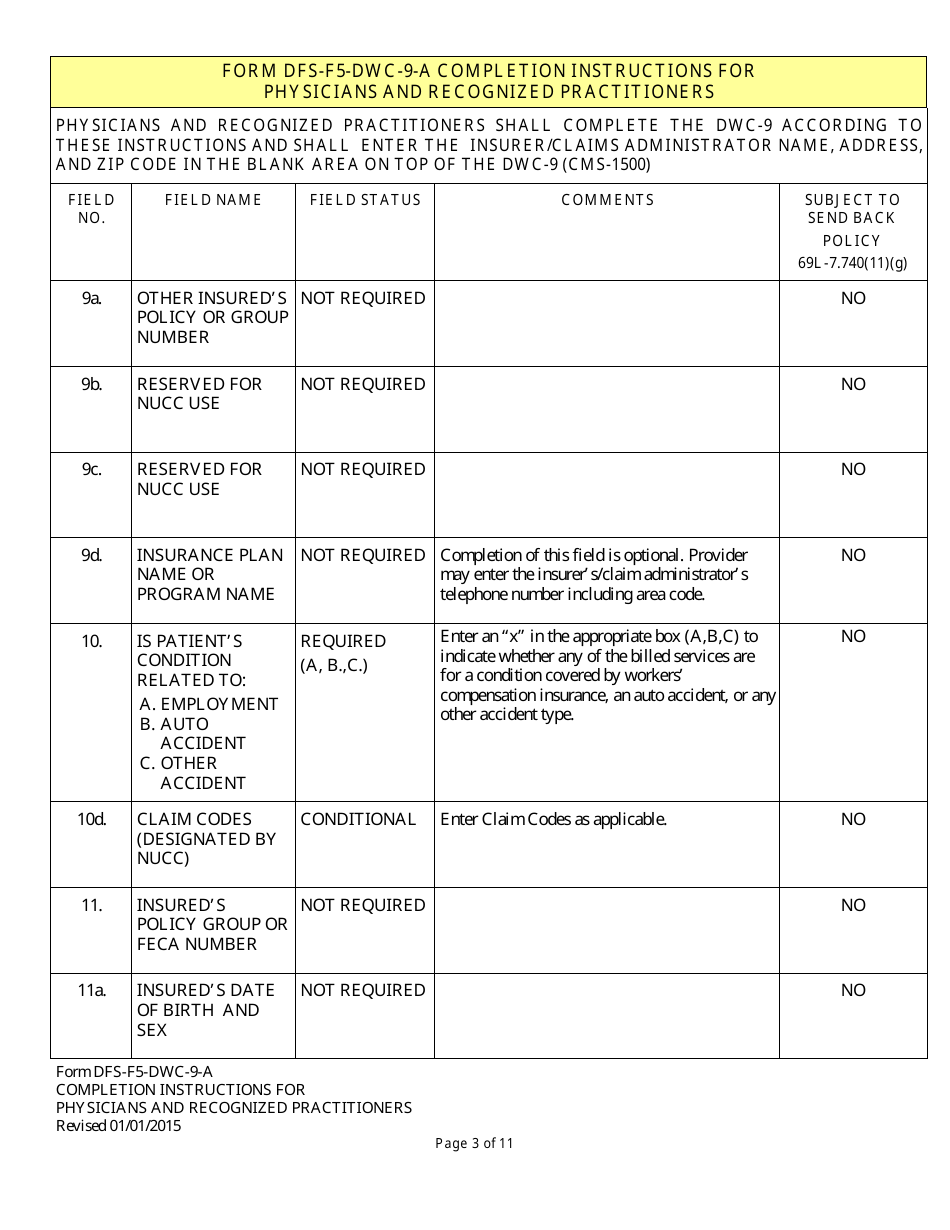
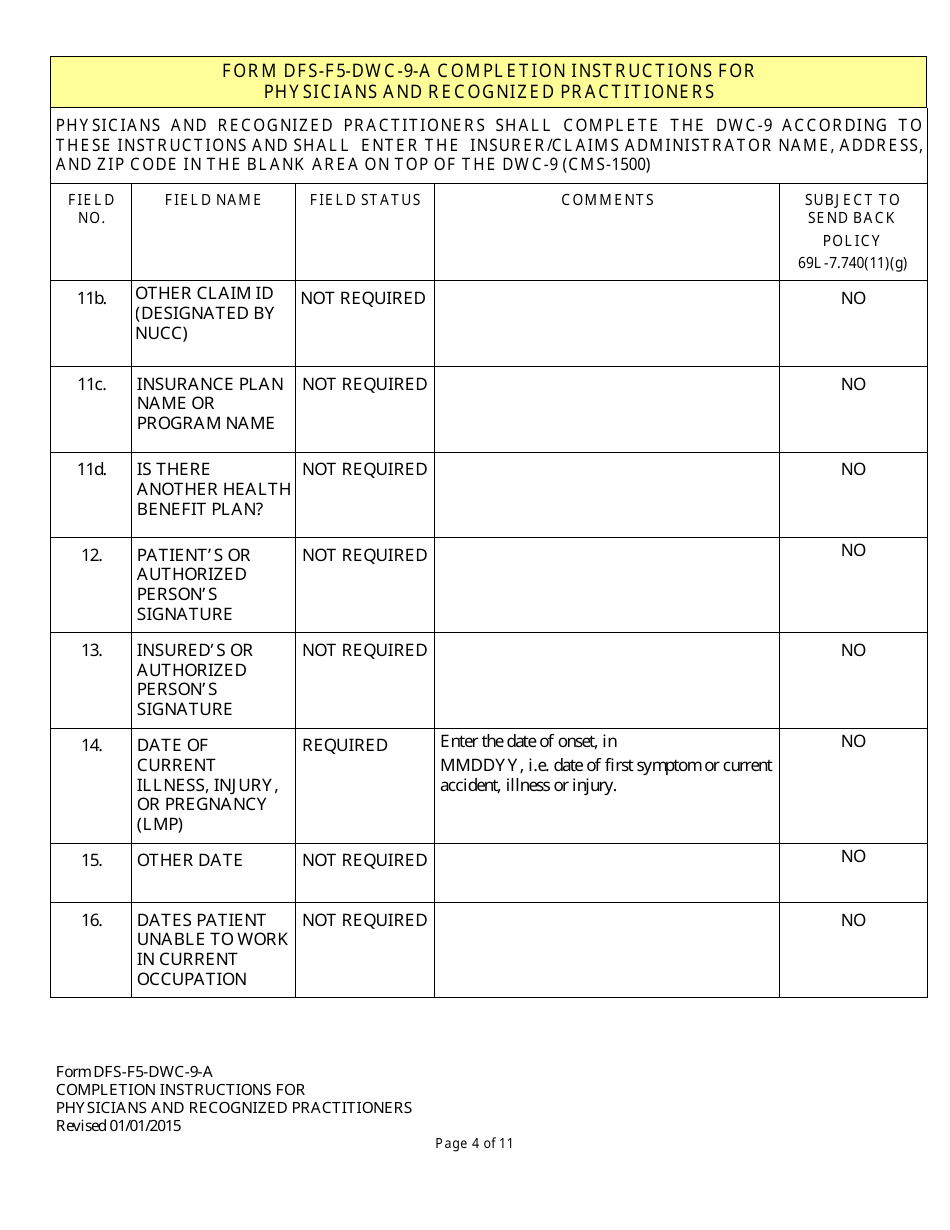
A: The form requires information such as patient demographics, insurance information, description of services, diagnosis codes, and billing details.
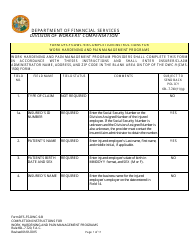
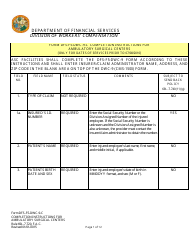
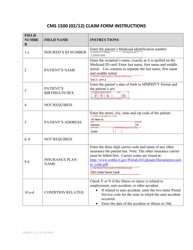
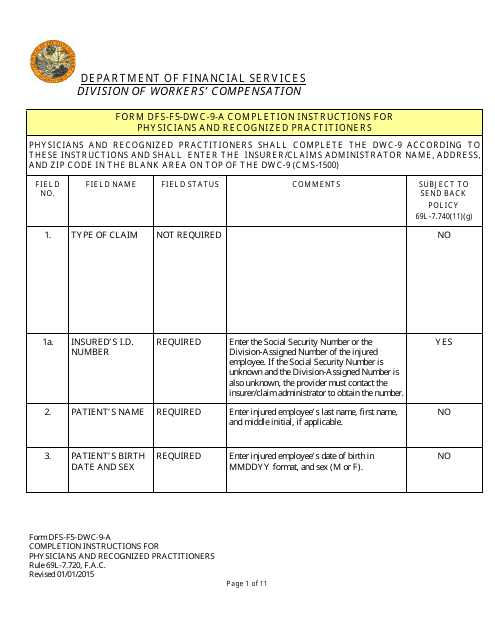
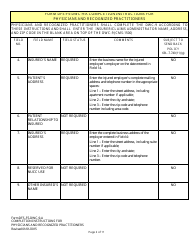
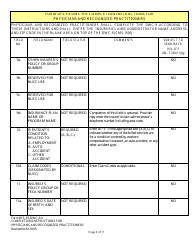
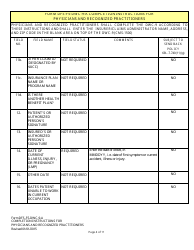
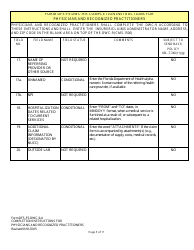
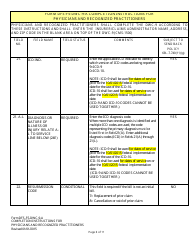
Q: Are there any instructions for completing this form?
A: Yes, there are instructions provided with the form that explain how tofill out each section accurately.
Q: Can I submit this form electronically?
A: Yes, you may be able to submit this form electronically depending on your health insurance company's guidelines.
Q: What should I do after completing this form?
A: After completing the form, you should submit it to your health insurance company for processing and payment.
Instruction Details:
- This 11-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the Florida Department of Financial Services.
Download Instructions for Form DFS-F5-DWC-9 Health Insurance Claim Form (Licensed Health Care Providers) - Florida
1
2
3
4
5
6
7
8
9
10
11