Form 2015 Verification of Medicaid Transportation Abilities - New York
What Is Form 2015?
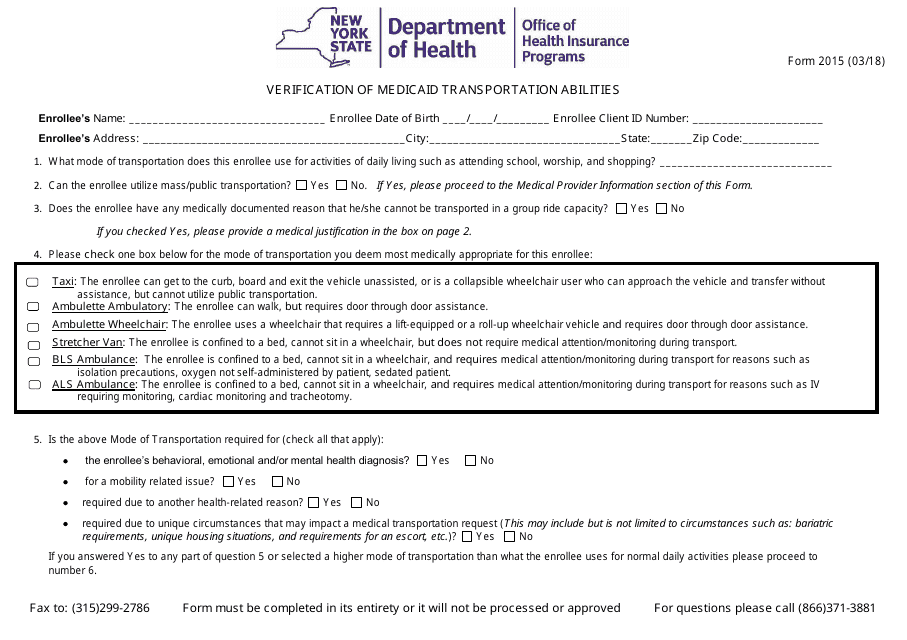
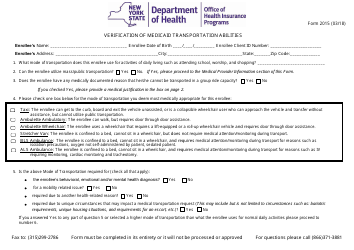
Form 2015, Verification of Medicaid Transportation Abilities , is a formal document used by New York residents to request a specific mode of transportation which is necessary because they are unable to use public transportation to go to school, places of worship, and stores. The state will approve the request for non-emergency transportation suitable if the applicant's attending physician confirms they need it because of the disability or illness that does not let them use traditional transportation.
Alternate Name:
- Medicaid Transportation Form.
This document was issued by the New York State Department of Health . The latest version of the form became available on March 1, 2018 , with all previous editions obsolete. You may download a Medicaid Transportation Form through the link below.
Medicaid Transportation Form Instructions
Here is how you need to prepare Form 2015:
- Enter the name, date of birth, and the address of the enrollee. Indicate the number they use to access Medicaid services.
- Write down the mode of transportation the enrollee uses every day.
- Answer "yes" if the applicant uses public transportation. Only declare the necessity for a specific form of non-emergency transportation if you answer "no".
- Confirm the enrollee cannot use a group ride transportation and describe the reasons on the second page of the form.
- Check the appropriate box to select the mode of transportation you require. Every option contains a short description - choose the one applicable to your health situation.
- Certify the transportation is needed because of the applicant's mental health issues, mobility-related condition, another health-related issue, or their living conditions.
- Record all mental and physical conditions that prevent the enrollee from using standard transportation. If you do not elaborate on these issues, the form may be rejected.
- State for how long the applicant will require the mode of transportation selected in the form.
- Certify the details in the report are true and complete. The medical provider must write down their name, National Provider Identifier number, add the contact information of their facility or clinic, and record the date of the request. Sign and date the form.
- Since Form 2015 is often prepared by the legal representative of the enrollee, it is also necessary to indicate the name and title of the individual who filled out the report.
Download Form 2015 Verification of Medicaid Transportation Abilities - New York
1

2