California Department of Health Care Services Forms
Documents:
1049
This Form is used for requesting to restrict the use and disclosure of protected health information for the Genetically Handicapped Persons Program in California.
This form is used for requesting information about the disclosure of protected health information in the Southern California Regional Office of the City of Los Angeles, California.
This form is used to request an accounting of the disclosures of protected health information made by the Genetically Handicapped Persons Program in the City of Sacramento, California.
This form is used for requesting to amend protected health information at the Sacramento Regional Office in the City of Sacramento, California.
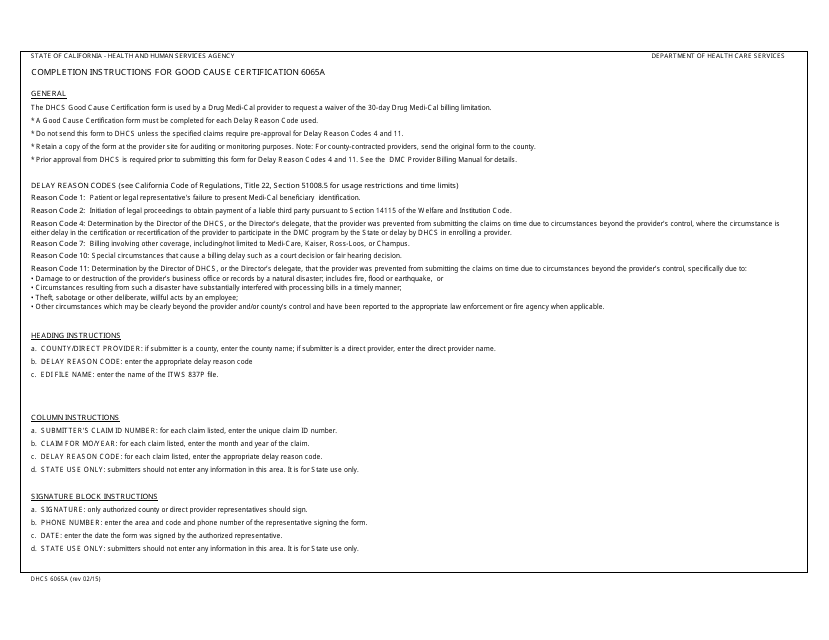
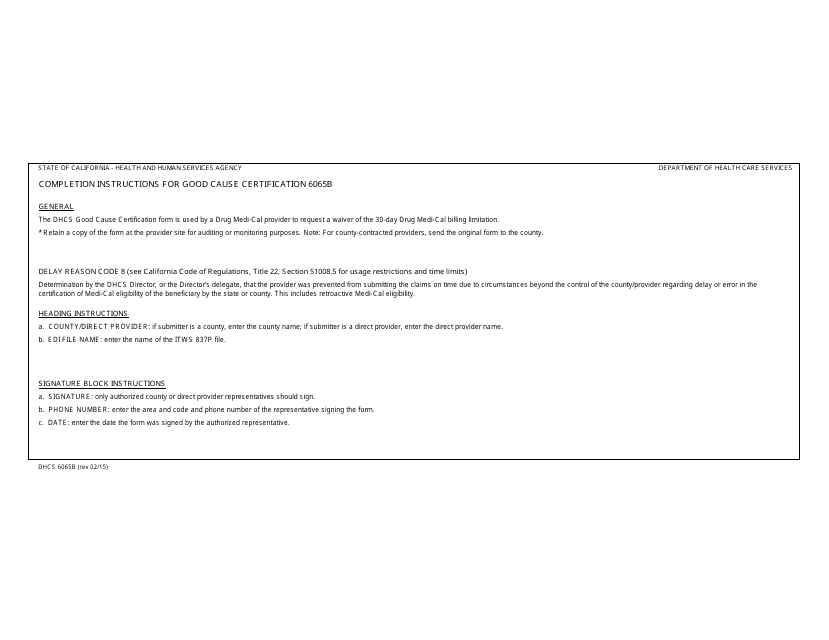
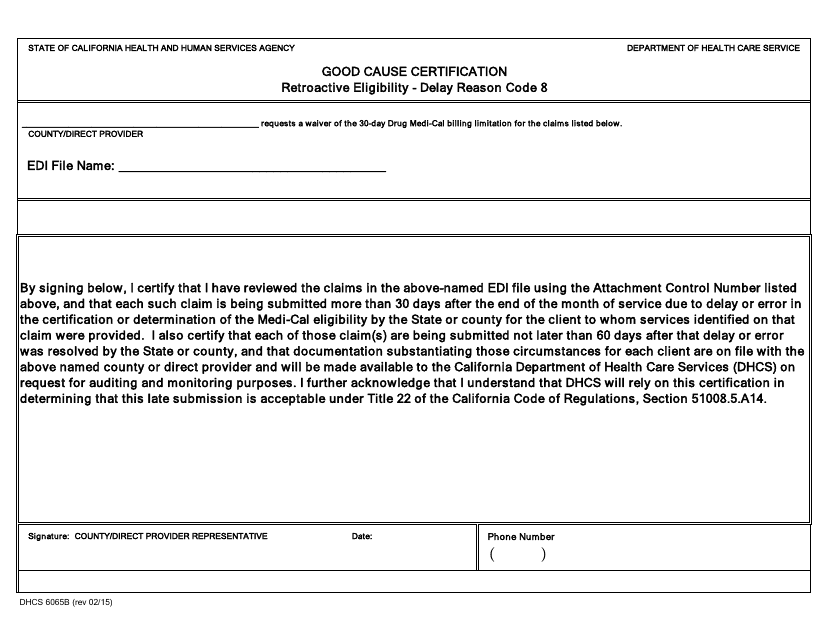
This form is used for requesting a good cause certification in California, which allows individuals to qualify for certain healthcare programs or exemptions.
This form is used for California county contracted providers to certify their submission of Drug Medi-Cal (DMC) claims.
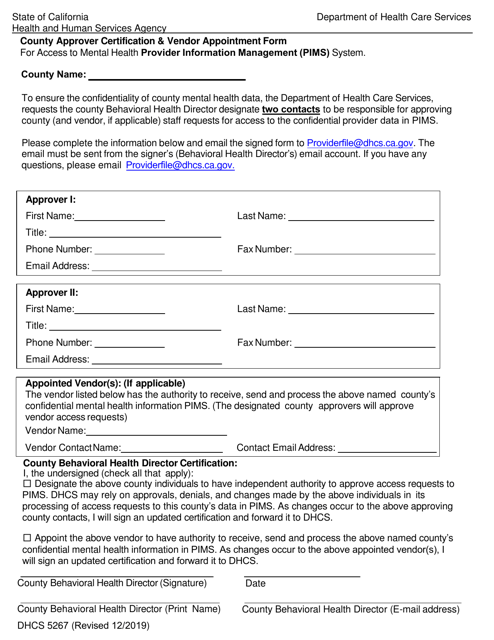
This form is used for obtaining employee approver certification in California under DHCS (Department of Health Care Services).
This Form is used for canceling the county/direct provider user registration in California.
This form is used for Drug Medi-Cal certification in California to seek federal reimbursement for drug treatment services.
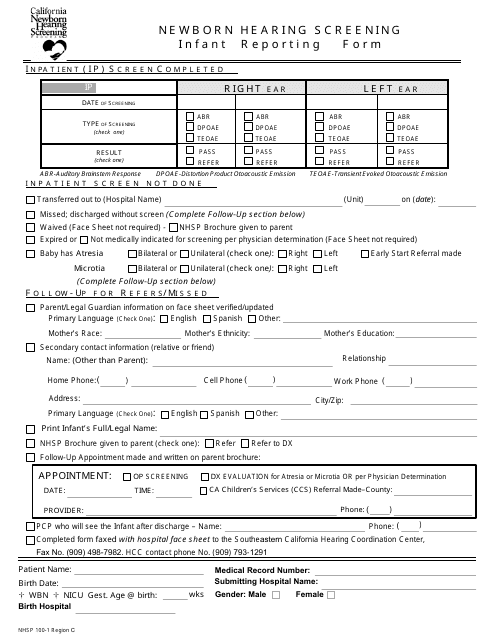
This form is used for reporting infant-related information in Region C of California.
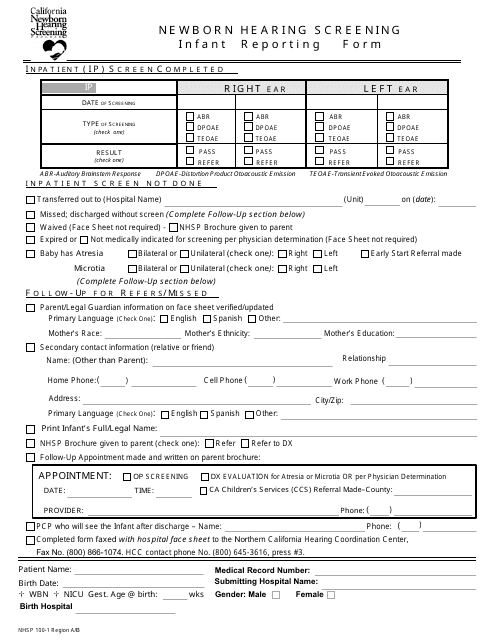
This form is used for reporting information about infants in Region a/B of California.
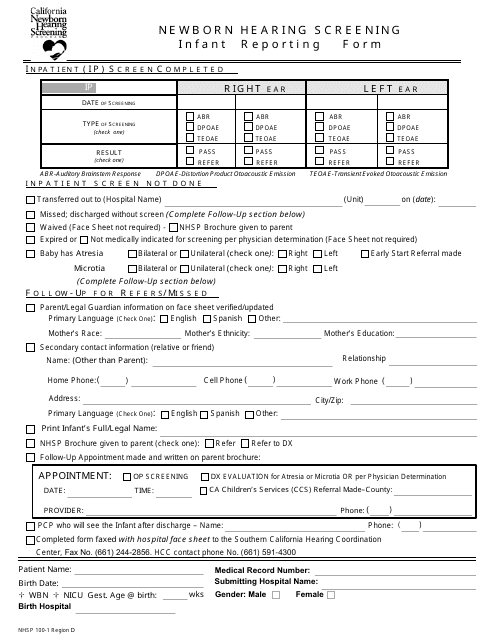
This form is used for reporting information related to infants in Region D, California.
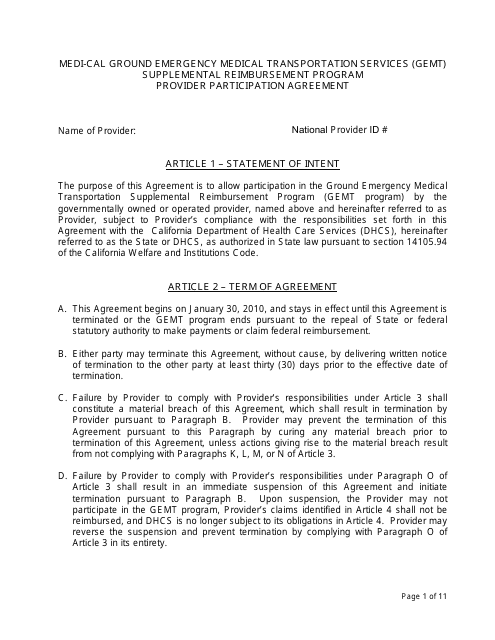
This Form is used for healthcare providers in California to participate in the Medi-Cal Ground Emergency Medical Transportation Services (GEMT) Supplemental Reimbursement Program.
This form is used for requesting a waiver for hearing screening in California.
This document provides the point of contact information for ground emergency medical transportation in California.