California Department of Health Care Services Forms
Documents:
1049

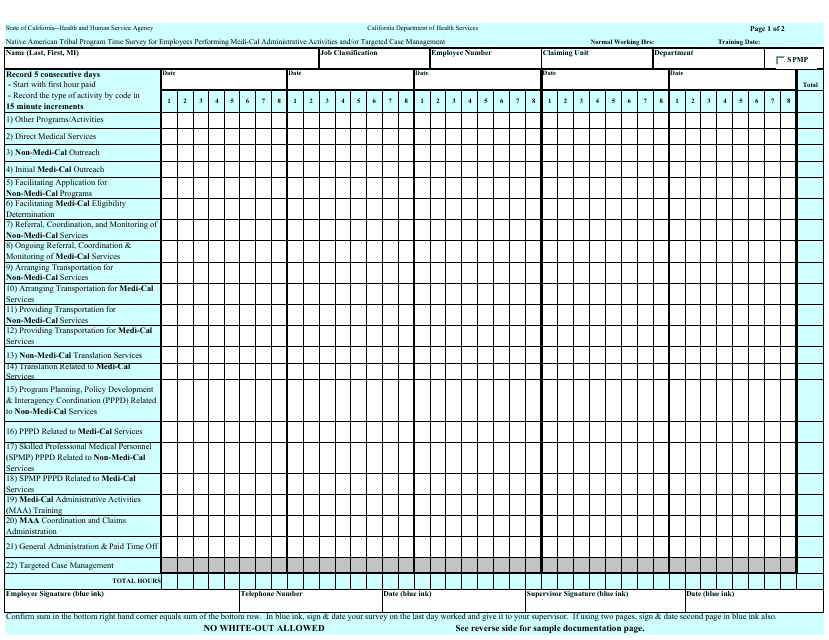
This form is used for Native American tribal program employees in California who perform Medi-Cal administrative activities and/or targeted case management to track their time spent on these activities.

This form is used for Native American tribal program employees in California who perform Medi-Cal administrative and/or targeted case management. It is a time survey for recording the hours worked.
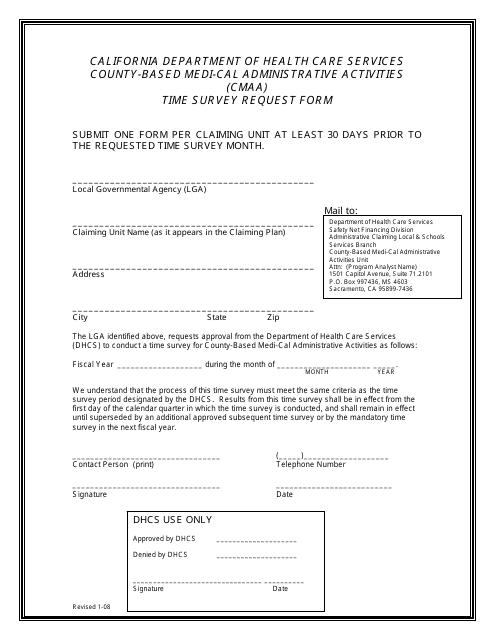
This form is used for reporting County-Based Medi-Cal Administrative Activities (CMAA) time survey data in California.
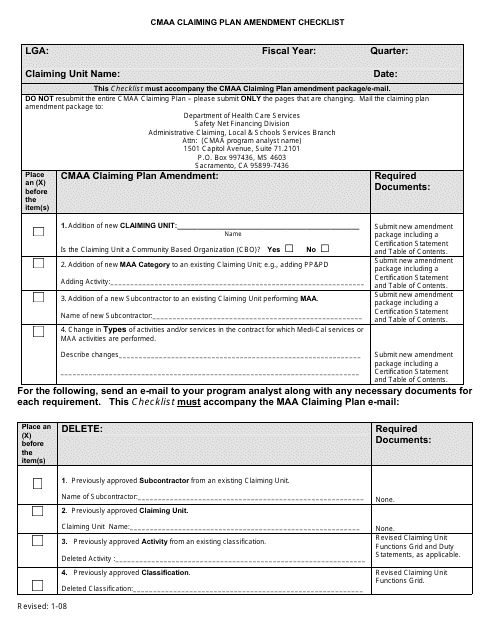
This document is used for the checklist of required amendments for claiming plan in the state of California. It helps ensure compliance with the CMAA regulations.
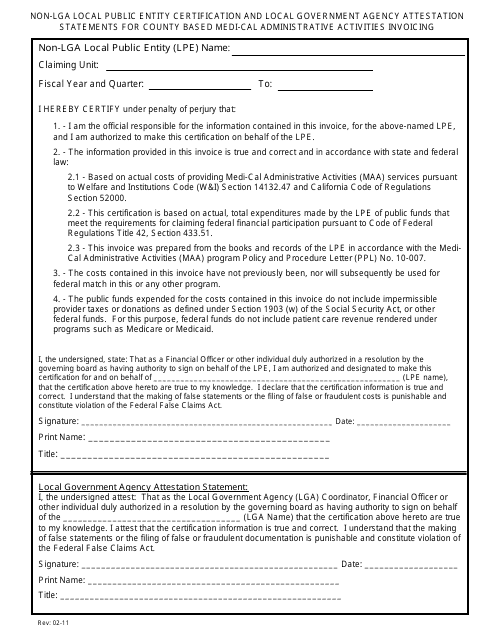
This document is used for certifying non-LGA local public entities and attesting statements for county-based Medi-Cal administrative activity invoicing in California.
This Form is used for the Genetically Handicapped Persons Program (GHPP) in California. It is a solicitud (application) to determine eligibility for the program for genetically disabled individuals.
This form is used for the pre-enrollment application for the Child Health and Disability Prevention (CHDP) Program in California. The form is available in Tagalog language.
This Form is used for Nutrition Screening for children aged birth to eight in California. It is available in Spanish.
This form is used for nutrition screening for children from birth to eight years old in California. It helps assess their dietary habits and nutritional needs.
This form is used for nutrition screening in California. It includes a food frequency questionnaire to assess dietary habits and nutritional needs.
This Form is used for screening nutrition in children and teenagers aged 8 to 19 in California. It is a frequency questionnaire conducted in Spanish.
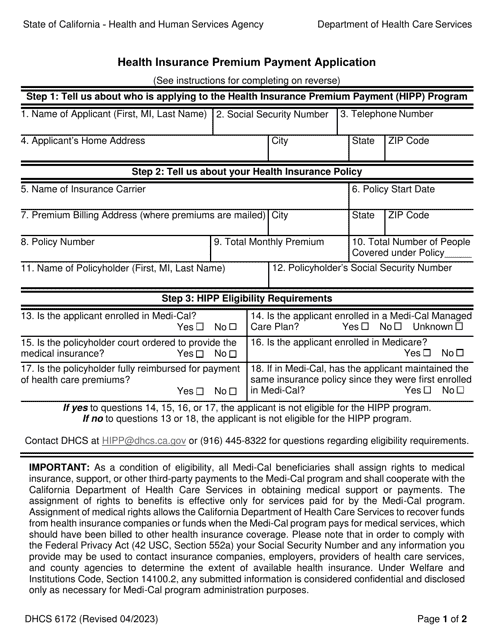
This type of document is used for applying for the Health Insurance Premium Payment (HIPP) program in California. It is a form written in Spanish.
This form is used for reporting the costs of care provided in Intermediate Care Facilities for the Developmentally Disabled (ICF-DDH/N) in California.
This Form is used for reporting the supplemental cost information related to Medi-Cal services in California.
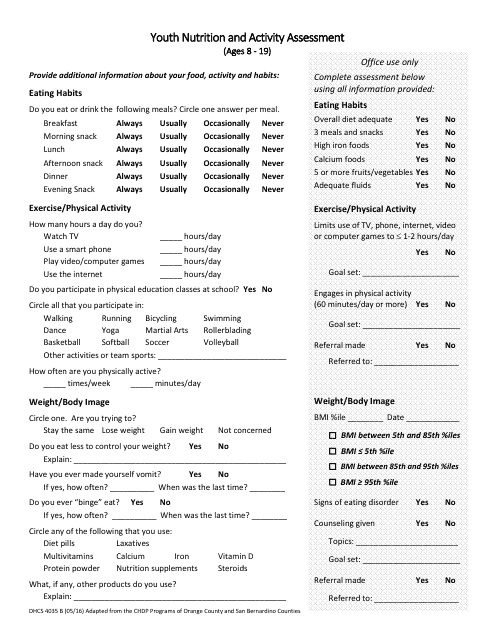
This form is used for Youth Nutrition and Activity Assessment for ages 8-19 in California. It helps in evaluating the dietary and physical activity practices of youth in the state.
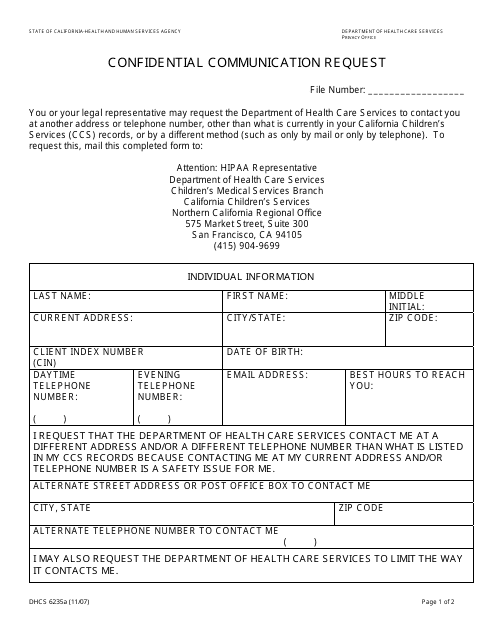
This form is used for submitting a confidential communication request to the Northern California Regional Office of the City and County of San Francisco, California.
This form is used for reporting the office costs of Intermediate Care Facilities for the Developmentally Disabled Habilitative/Nursing (ICF-DDH/N) homes in California.
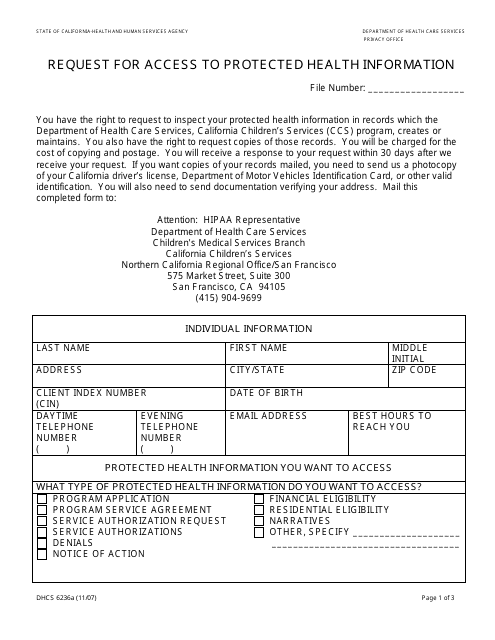
This form is used for requesting access to protected health information in the Northern California Regional Office/San Francisco of the City and County of San Francisco, California.
This Form is used for parents, guardians, or legal representatives in San Francisco to request access to protected health information for a child or dependent.
This form is used for requesting information about the disclosure of protected health information in the Northern California Regional Office/San Francisco. It can be filled out by a parent, guardian, or legal representative in the City and County of San Francisco, California.
This Form is used for requesting to amend protected health information by a parent, guardian, or legal representative in the San Francisco region of Northern California.
This form is used for requesting to restrict the use and disclosure of protected health information by a parent, guardian, or legal representative in the Northern California Regional Office/San Francisco area. It is specific to the City and County of San Francisco, California.
This form is used for requesting an accounting of disclosures of protected health information in the Northern California Regional Office/San Francisco.
This form is used for requesting confidential communication at the Southern California Regional Office of the City of Los Angeles, California.
This form is used for parents, guardians, or legal representatives in the Southern California Regional Office of the City of Los Angeles, California to request access to protected health information.
This form is used to request access to protected health information from the Sacramento Regional Office in the City of Sacramento, California.
This Form is used for requesting to restrict the use and disclosure of protected health information by a parent, guardian, or legal representative in the Southern California Regional Office of the City of Los Angeles, California.
This form is used to request access to protected health information from the Southern California Regional Office in the City of Los Angeles, California.
This document is a form used to request confidential communication with the Sacramento Regional Office in the City of Sacramento, California.
This Form is used for requesting to restrict the use and disclosure of protected health information for minors by their parent, guardian or legal representative in Sacramento, California.
This form is used for requesting information about the disclosure of protected health information in the Sacramento Regional Office of the City of Sacramento, California.
This form is used for requesting restrictions on the use and disclosure of protected health information in the Sacramento Regional Office of the City of Sacramento, California.
This form is used for requesting information about the disclosure of your protected health information by the Southern California Regional Office of the City of Los Angeles, California.
This form is used for requesting to amend protected health information in the Genetically Handicapped Persons Program (GHPP) in California.
This form is used for parents, guardians, or legal representatives to request access to protected health information for individuals in the Genetically Handicapped Persons Program in the City of Sacramento, California.
