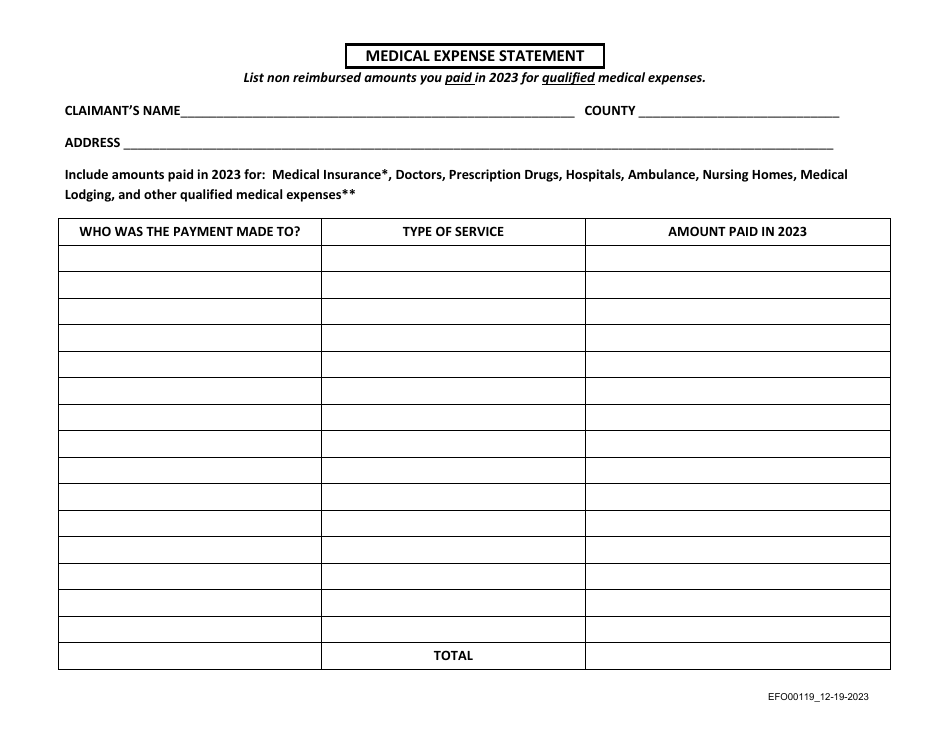
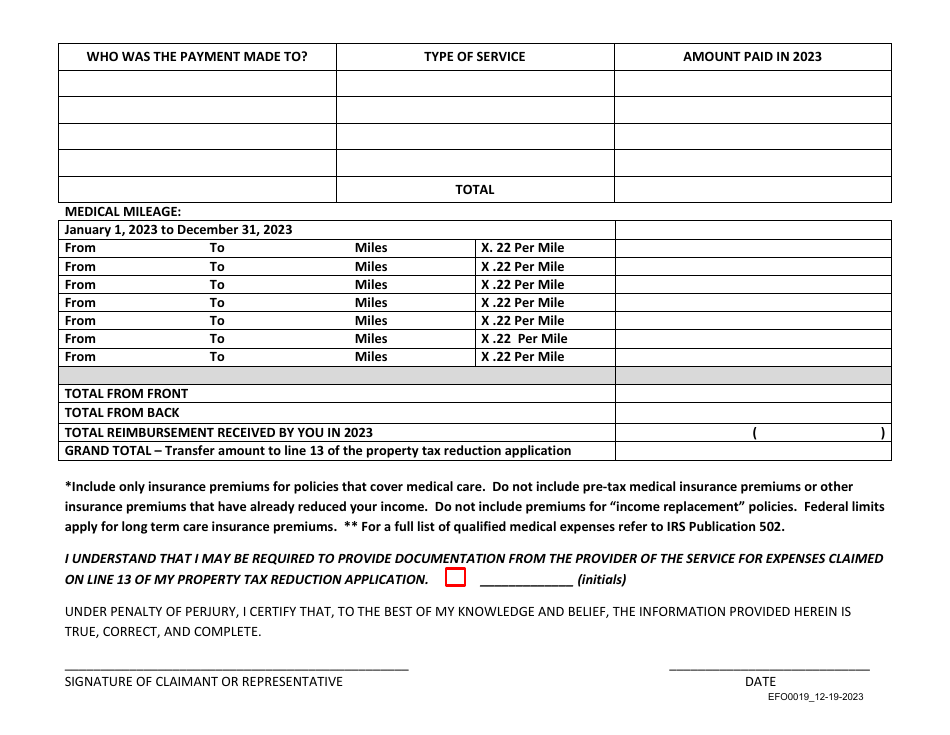
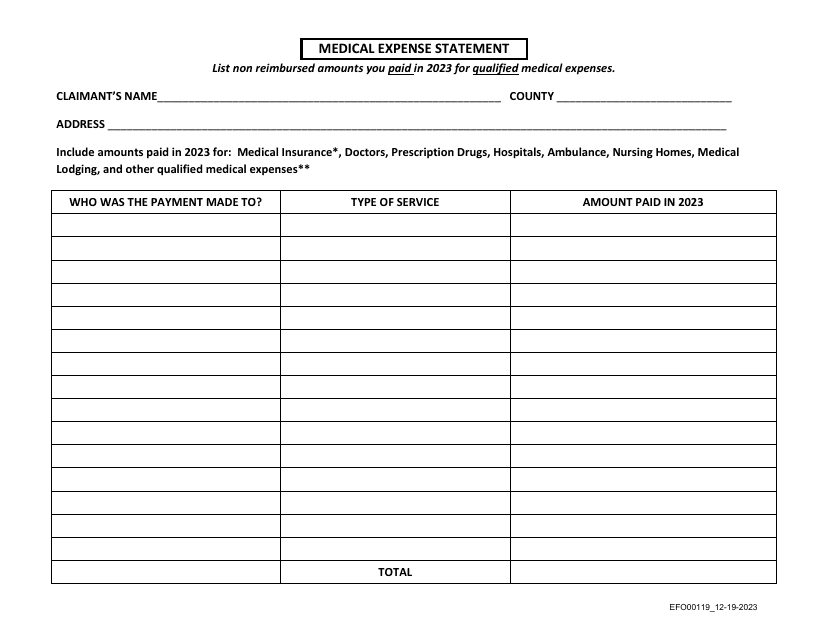
Form EFO00119 Medical Expense Statement - Idaho
Fill PDF Online
Fill out online for free
without registration or credit card
Other Revision
Download Form EFO00119 Medical Expense Statement - Idaho
1
2