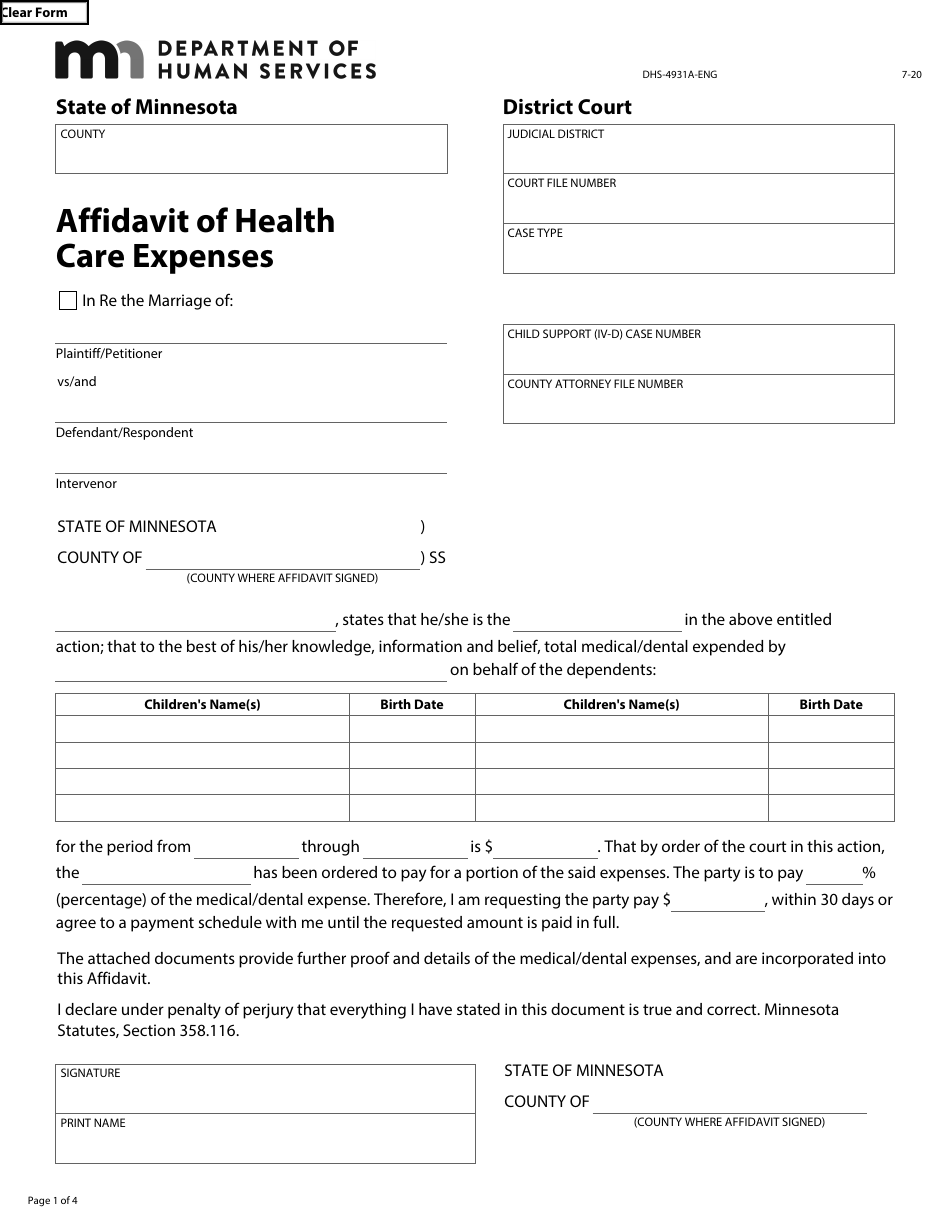
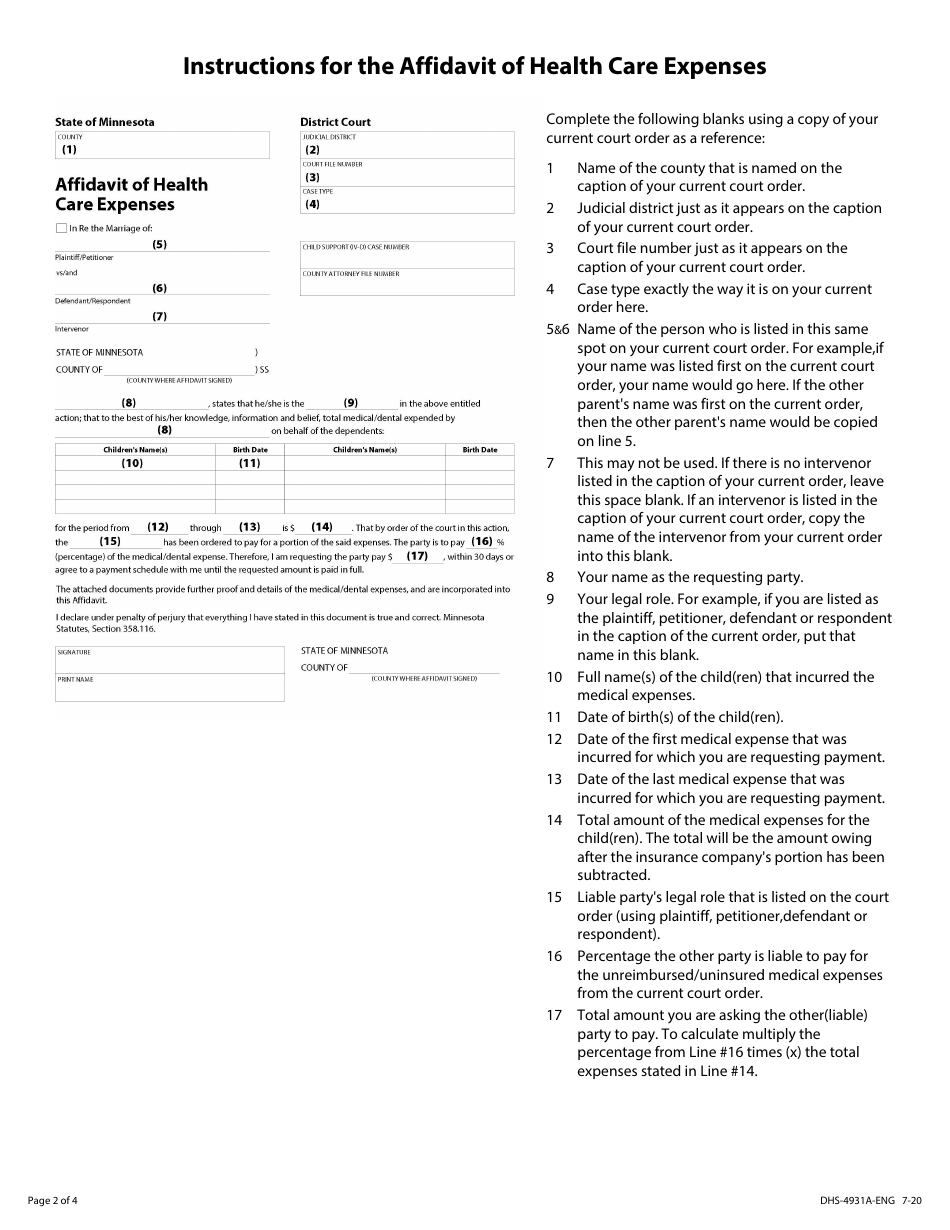
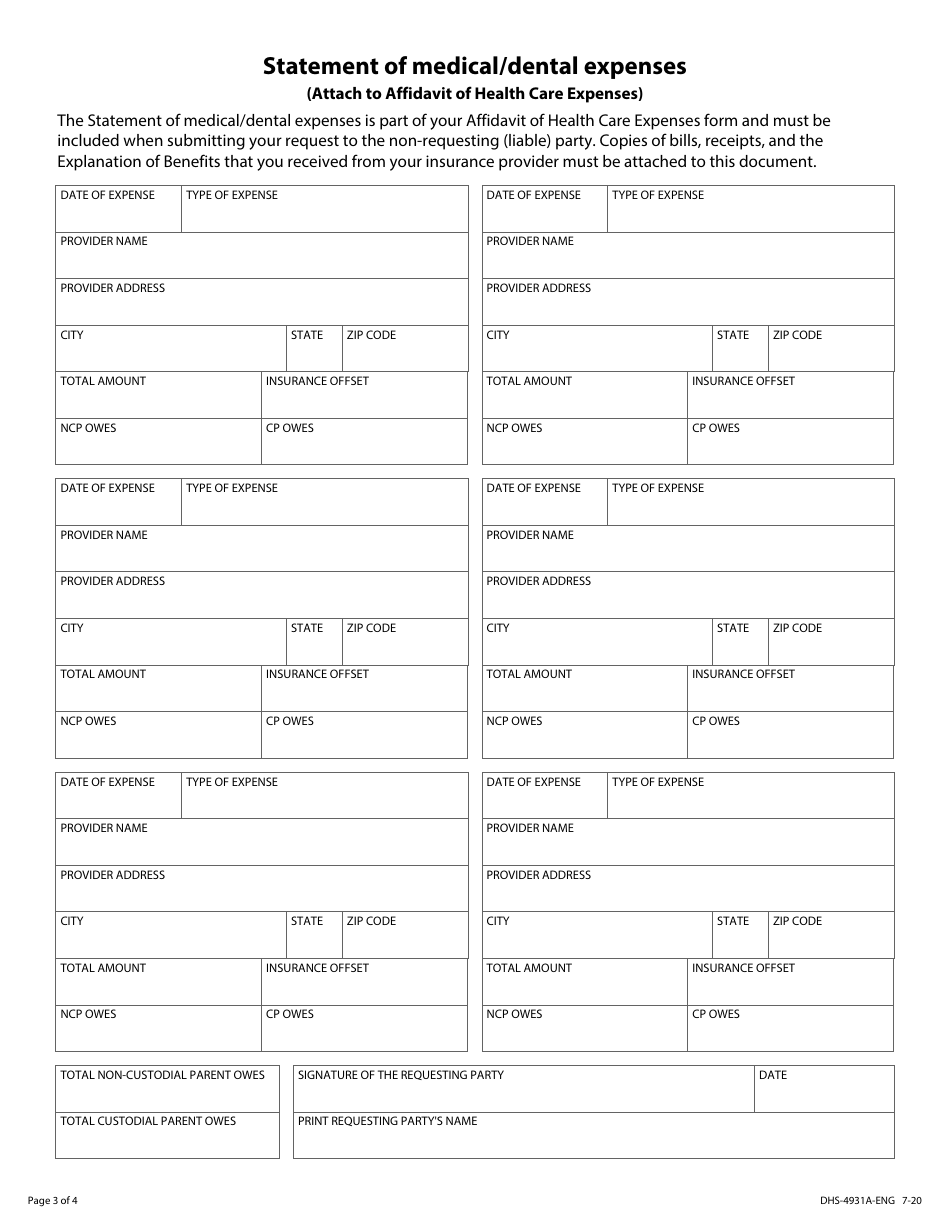
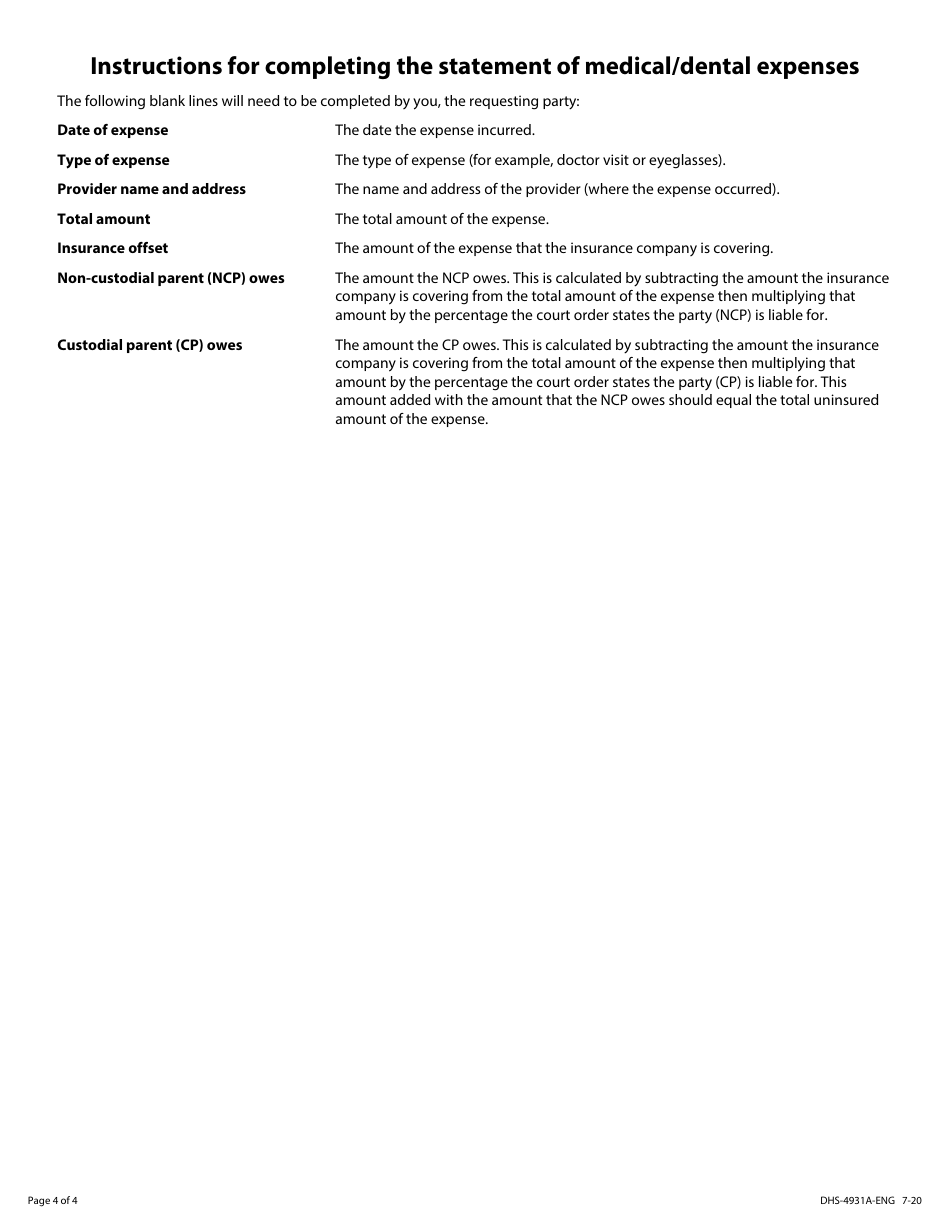
Form DHS-4931-ENG Unreimbursed and / or Uninsured Medical / Dental Expenses Packet - Minnesota
Fill PDF Online
Fill out online for free
without registration or credit card
Other Revision
Download Form DHS-4931-ENG Unreimbursed and / or Uninsured Medical / Dental Expenses Packet - Minnesota
1

2

3

4
5

6

7

8
9