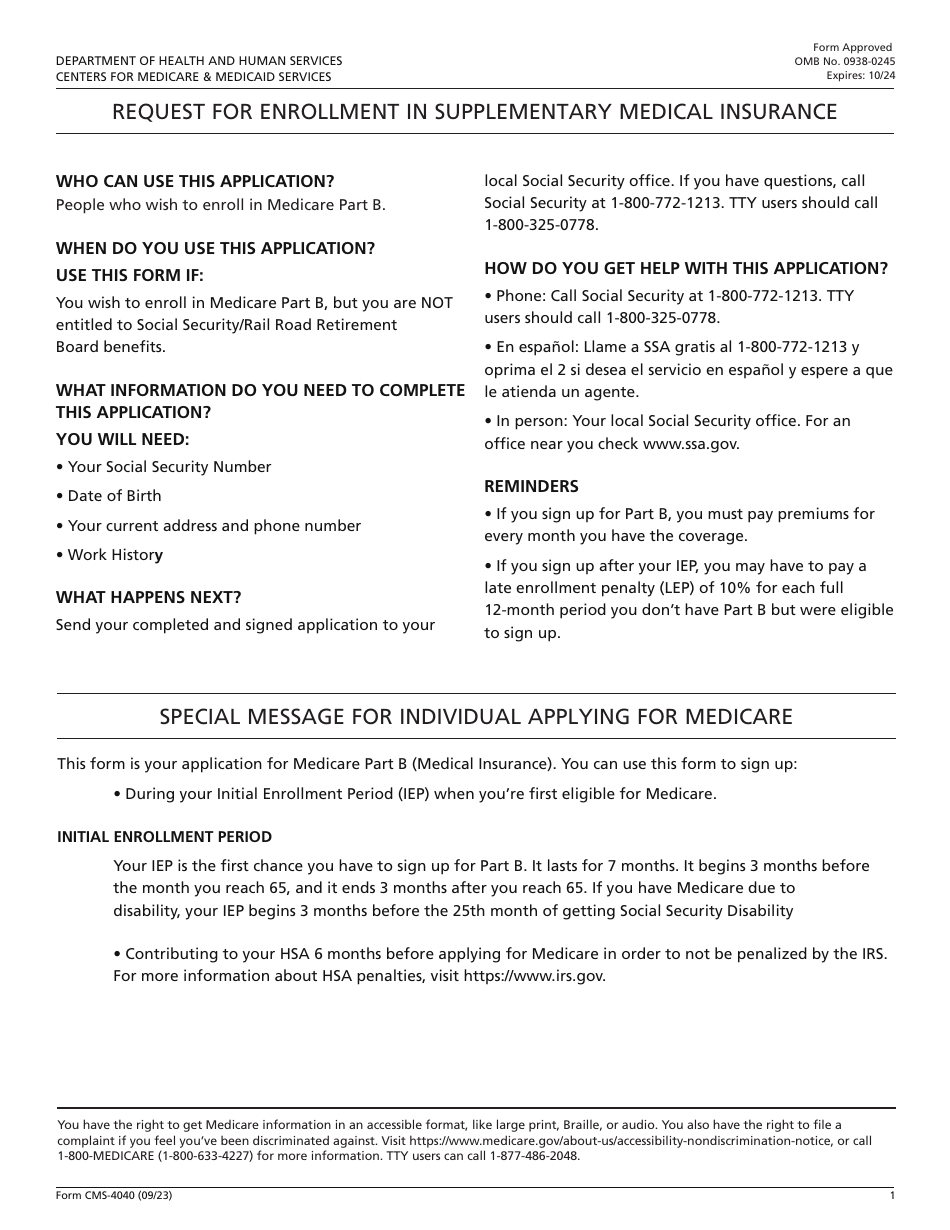
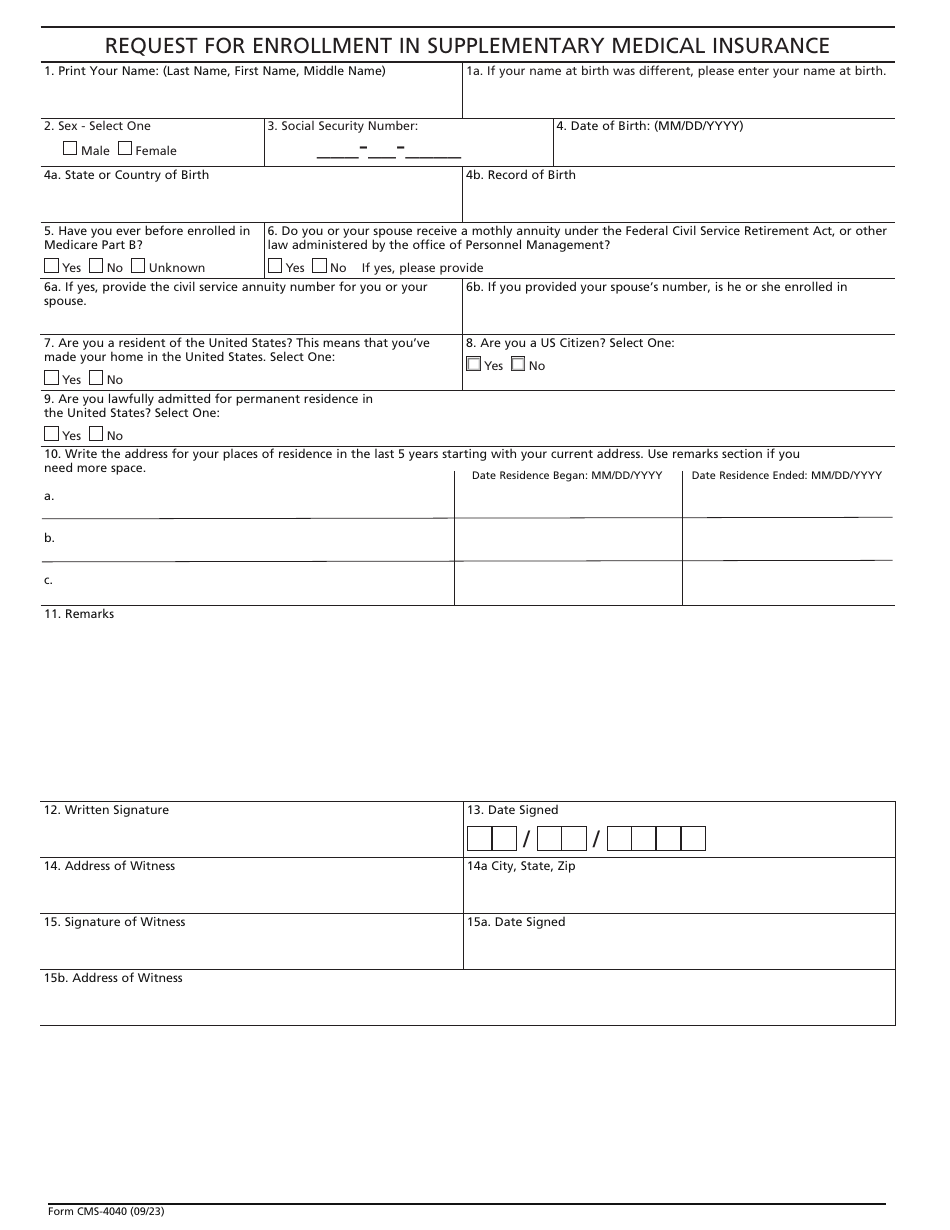
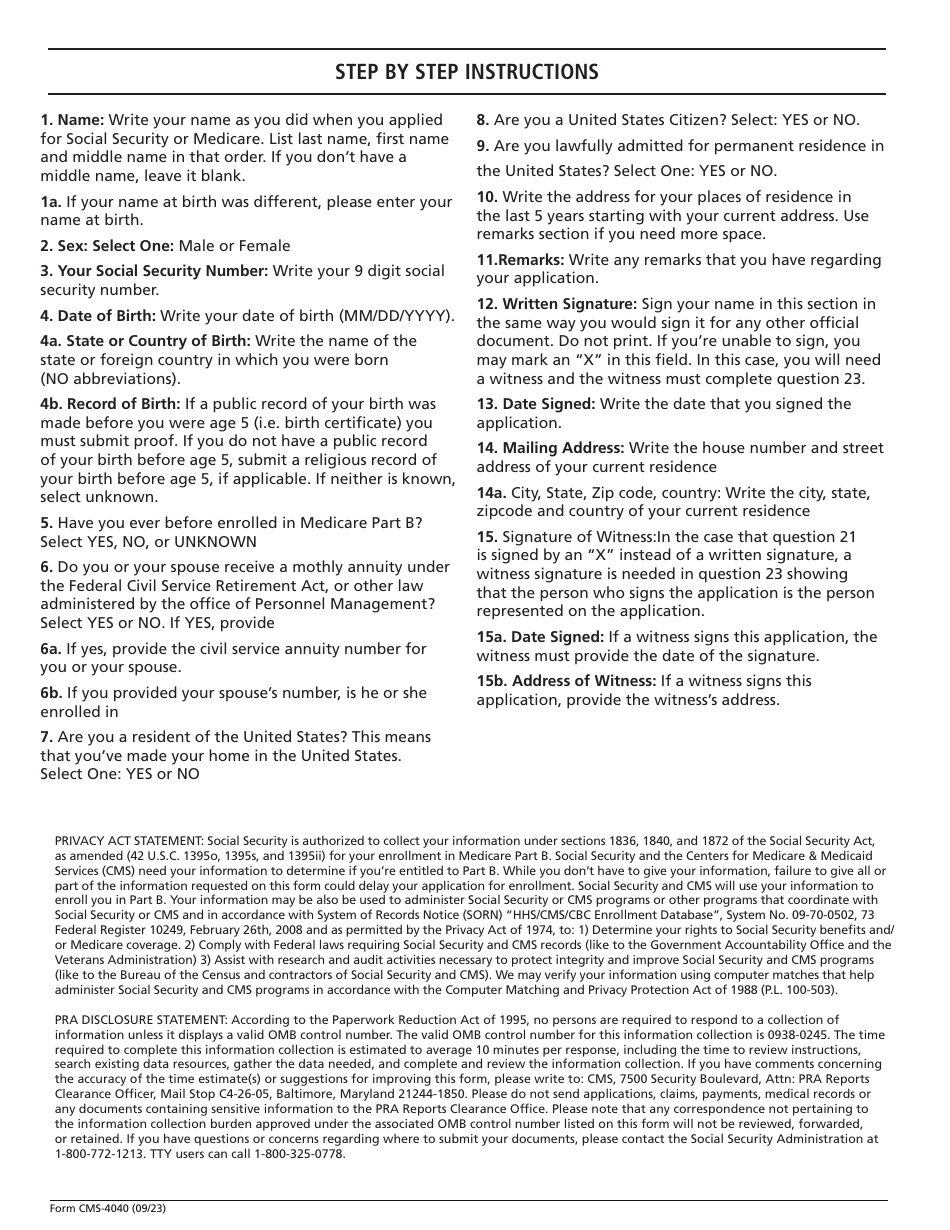
Form CMS-4040 Request for Enrollment in Supplementary Medical Insurance
Fill PDF Online
Fill out online for free
without registration or credit card
Other Revision
Download Form CMS-4040 Request for Enrollment in Supplementary Medical Insurance

1
2

3