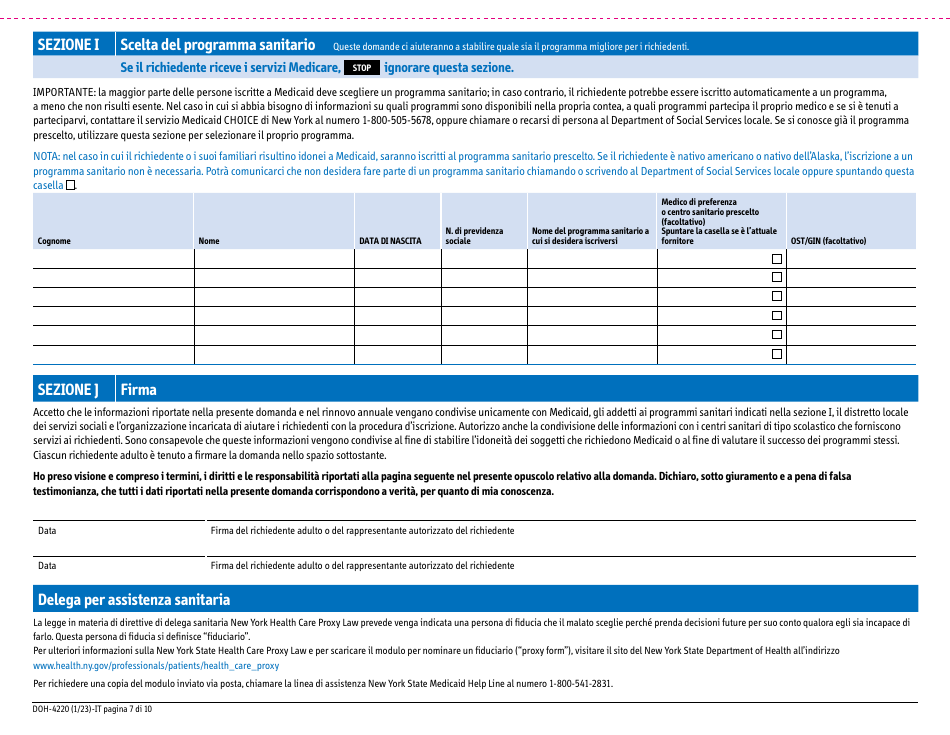
Form DOH-4220 Medicaid Application for Non-magi Eligibility Group - New York (Italian)

Fill PDF Online
Fill out online for free
without registration or credit card
Other Revision
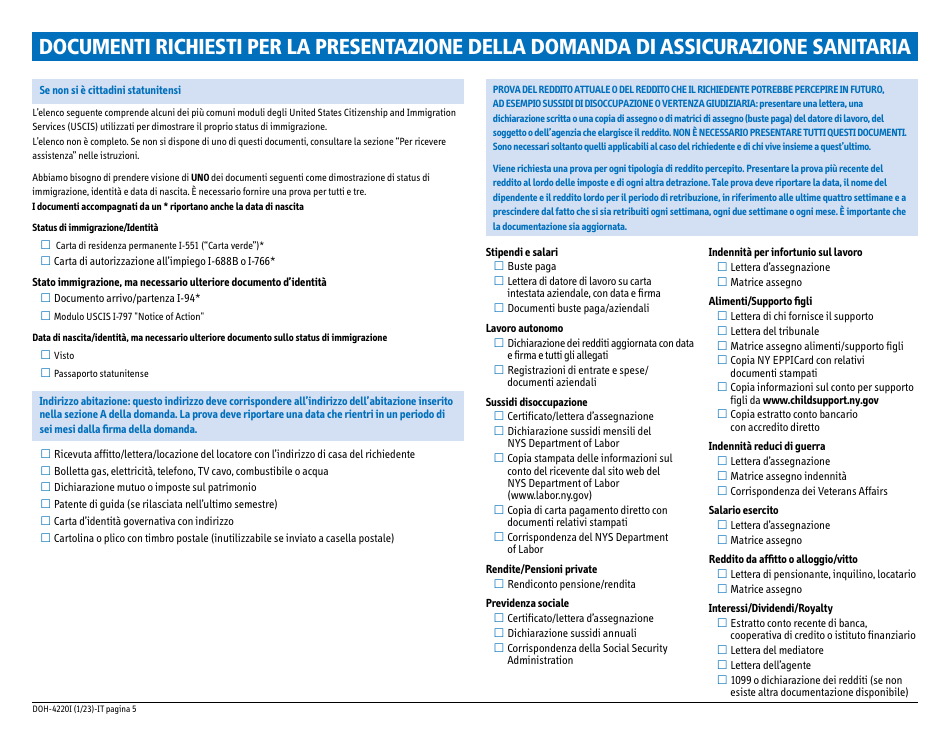
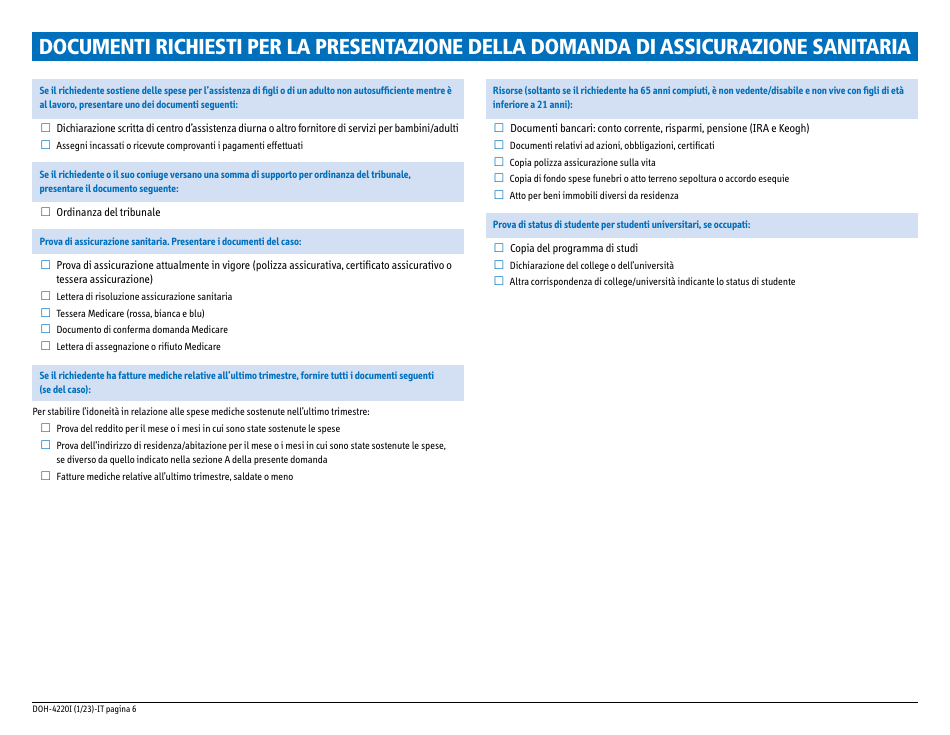
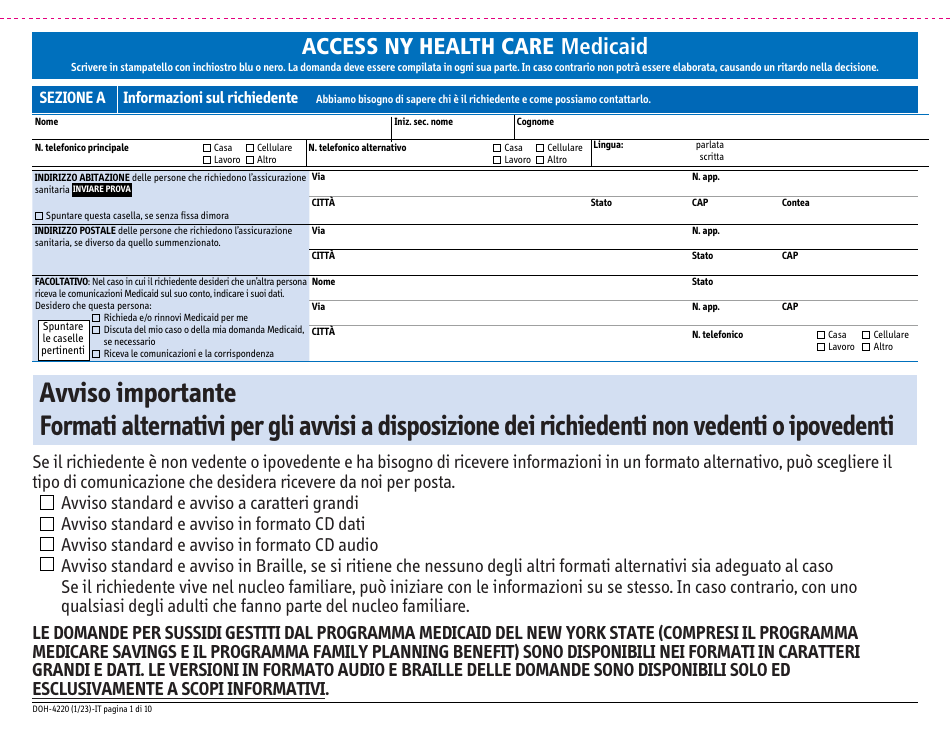
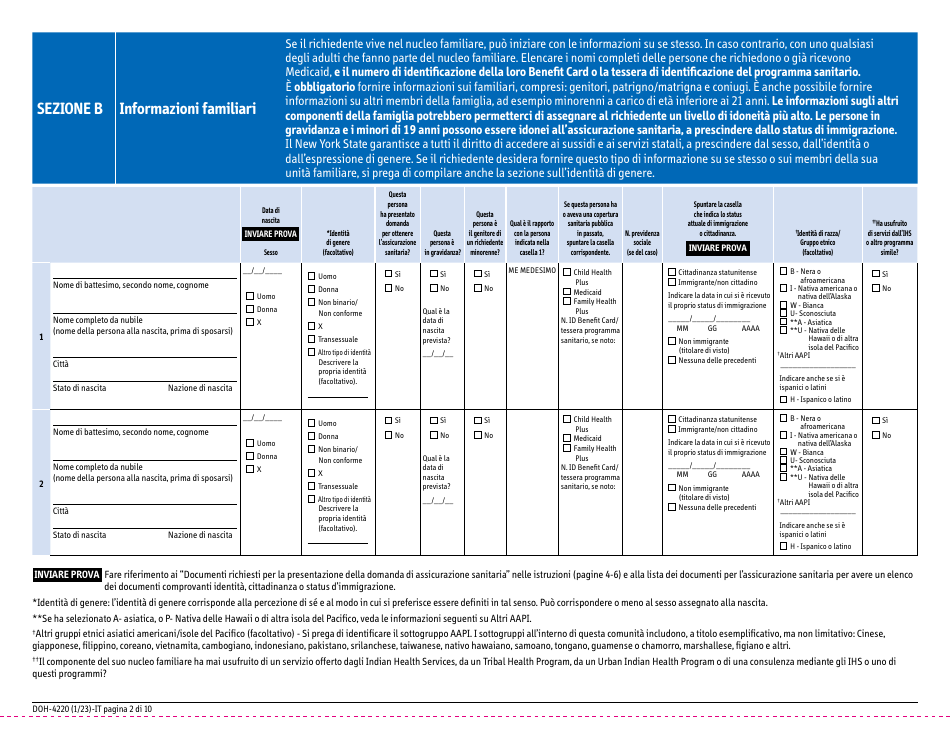
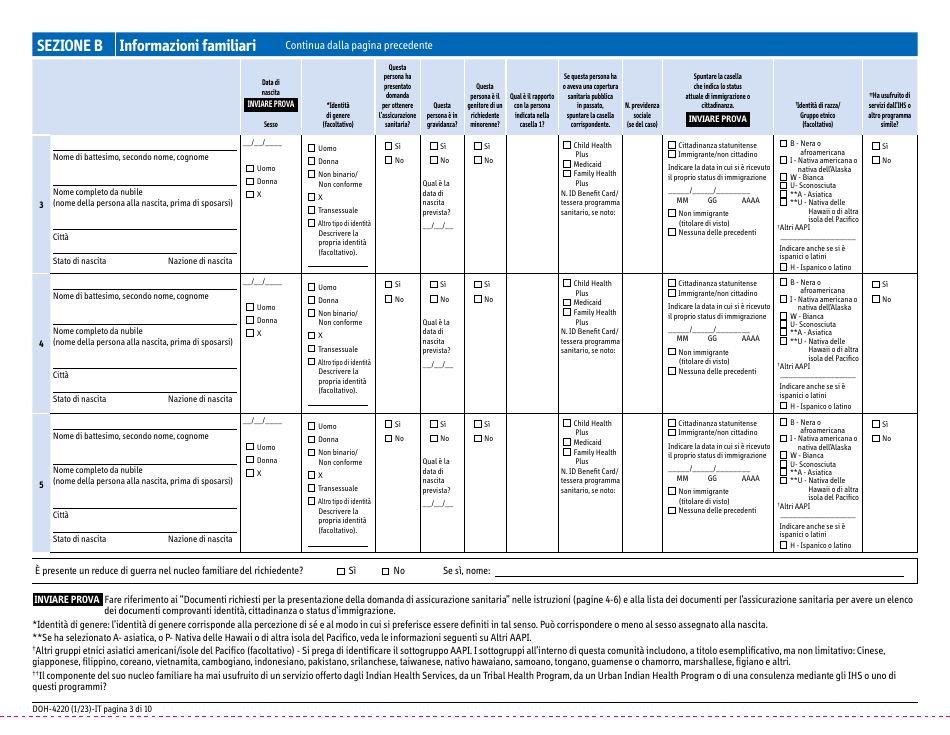
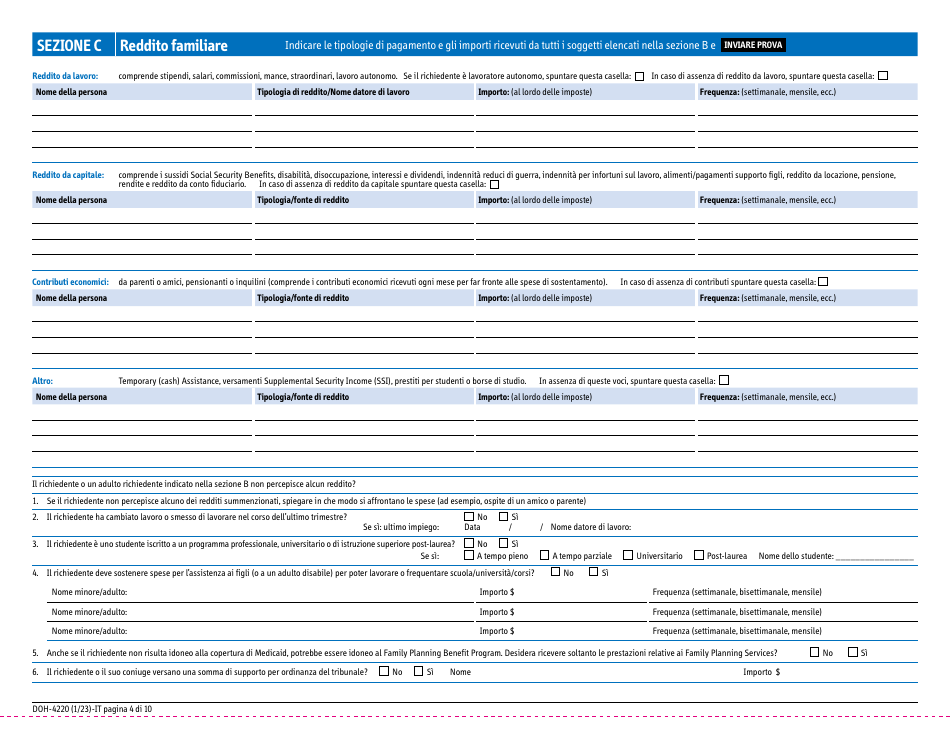
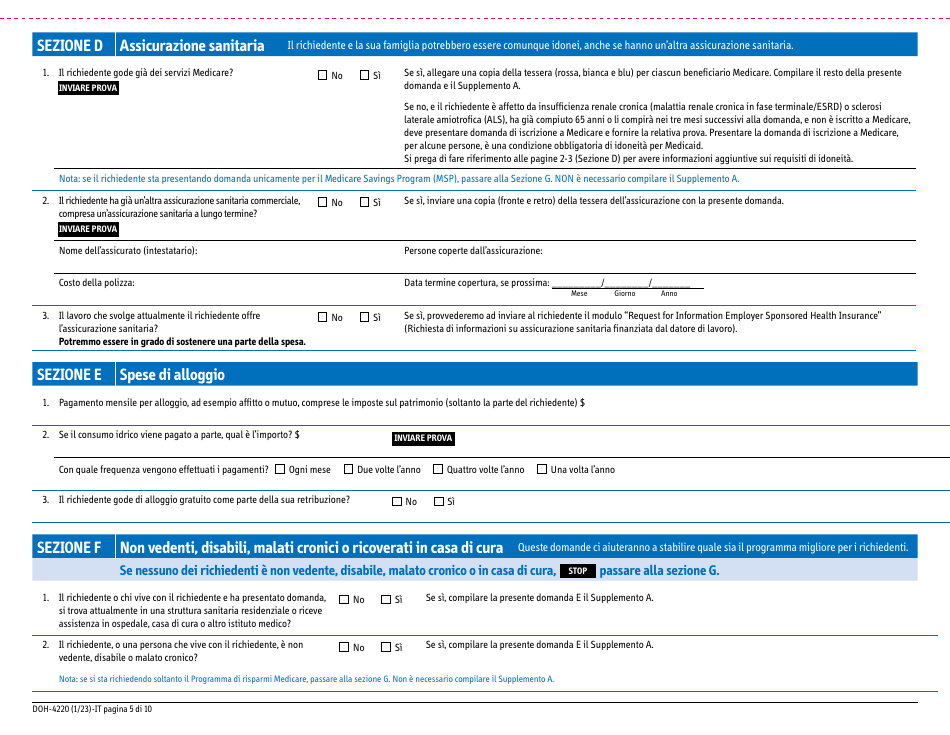
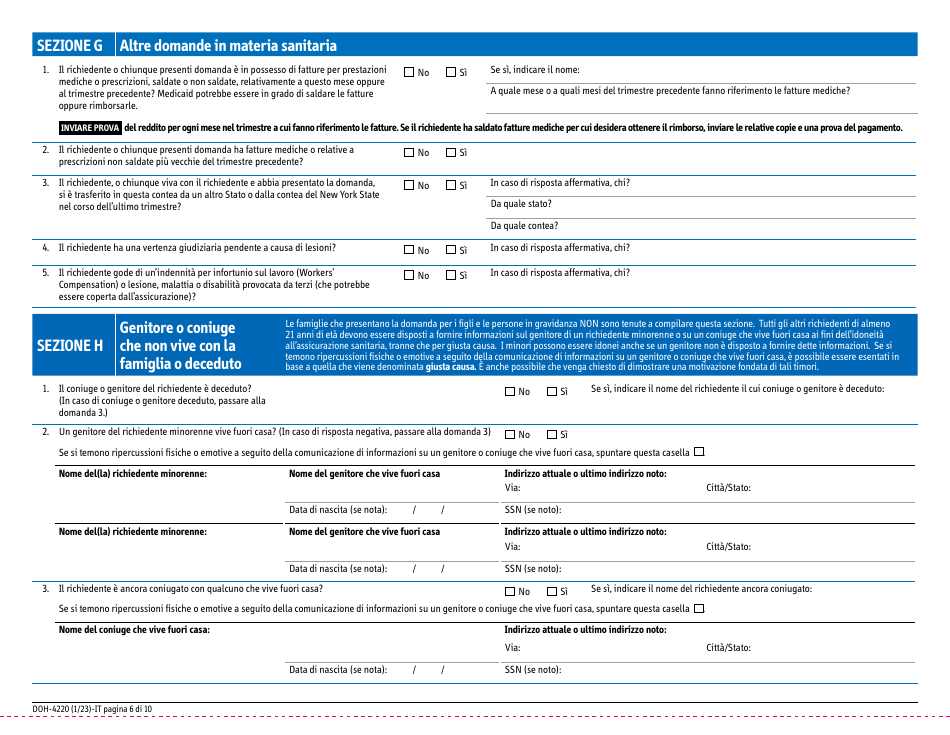
Download Form DOH-4220 Medicaid Application for Non-magi Eligibility Group - New York (Italian)

1

2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18

19
20