Form CMS-1763 Request for Termination of Premium Part a, Part B, or Part B Immunosuppressive Drug Coverage
What Is Form CMS 1763?
Form CMS-1763, Request for Termination of Premium Hospital and/or Supplementary Medical Insurance , is a legal document that any Medicare enrollee may use to terminate hospital insurance (Medicare Part A) and supplementary medical insurance (Medicare Part B). If you are enrolled in Medicare and wish to voluntarily stop your Medicare coverage, complete a CMS-1763 Form.
This form was released by the U.S. Department of Health and Human Services . You can download a fillable Form CMS 1763 through the link below.
How to Complete Form CMS 1763?
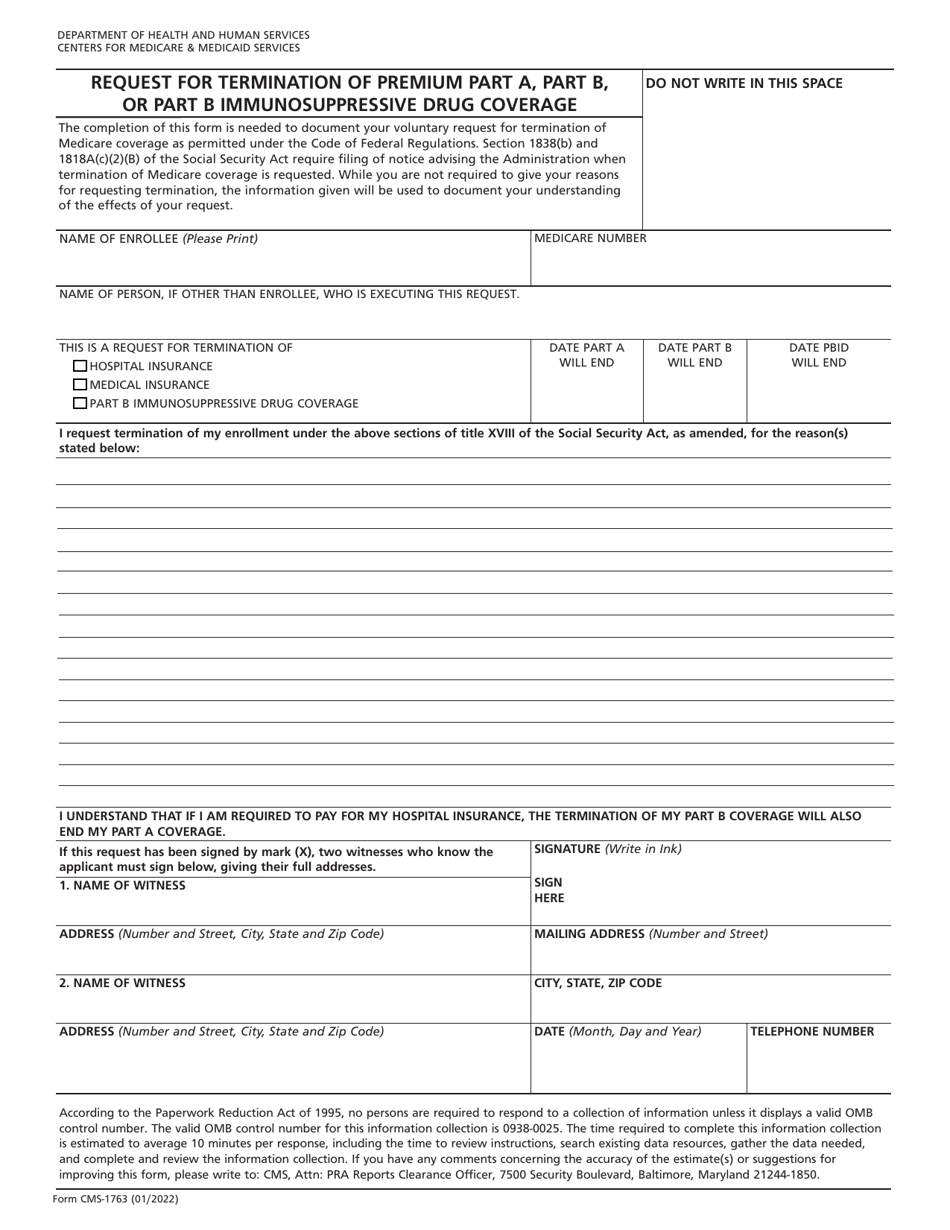
CMS 1763 instructions are as follows:
- Write down the name of the enrollee. If another individual executes this request, write down this person's name also;
- State your Medicare number;
- Choose the type of coverage you want to terminate. You may select either hospital insurance (Plan A) or medical insurance (Plan B), or withdraw from both if you desire so;
- Indicate the date when your hospital or medical insurance coverage should end;
- State the reasons for the termination. Give as many details as you wish. This request is most often made after an individual or their spouse finds a job that offers lifetime insurance. You are allowed to go into as much detail as you want, for instance, if you received a job with health insurance benefits, describe this job, indicate the type of benefits, and name your new insurance company. The information given will be used to document your understanding of the consequences of the withdrawal;
- Make sure the request is complete and sign the form. Your signature indicates that you understand the consequences of insurance coverage termination;
- Obtain signatures of two witnesses. They have to be familiar with the enrollee to be prepared to testify the applicant files the form in sound mind and body, while also making the best possible decision. The witnesses must sign the form, write down their names and addresses. Record the date of signing.
There is no due date or strict timeline regulations for the termination of your medical coverage. File this form when you deem it necessary - in any month and for any reason. However, you must know the termination will not take place until the end of the month in which you submitted the papers.
Where to Mail Form CMS-1763?
You are required to submit Form CMS-1763 to the nearest Social Security Administration (SSA) office. The disenrollment request will not be accepted directly from individuals. Visit the office to speak with a Social Security representative and complete the document during or after a personal interview, since this is a serious decision. Before filing the form, you need to explain the reason for withdrawal and you will get an explanation for the procedure and consequences of this insurance termination. You may also call the SSA toll-free at 1-800-772-1213 to be interviewed, and the representative will fill out the form with the information you provide.
Other Revision
Download Form CMS-1763 Request for Termination of Premium Part a, Part B, or Part B Immunosuppressive Drug Coverage
1
2