![]() This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2527
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2527
for the current year.
DD Form 2527 Statement of Personal Injury - Possible Third Party Liability, Defense Health Agency
What Is DD Form 2527?
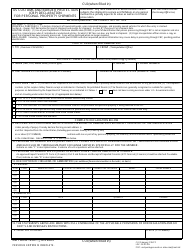
DD Form 2527, Statement of Personal Injury - Possible Third Party Liability is an Army form sent out by TRICARE to individuals whose medical expenses may have been a result of injuries caused by a third party.
The liable side may be an individual or a business. If their responsibility is proven, TRICARE will demand reimbursement for its medical costs under the Federal Medical Recovery Act.
The most recent version of the form - commonly referred to as the TRICARE DD Form 2527 - was released by the Department of Defense (DoD) on August 1, 2016, with all previous editions being obsolete. An up-to-date fillable DD Form 2527 is available for download and digital filing below or can be found on the Executive Services Directorate website.
Where to Mail DD Form 2527?
A copy of the DD Form 2527 will be sent by a regional TRICARE contractor to all individuals who meet any the following criteria:
- The medical treatment received exceeded $500;
- The patient was assigned a diagnosis code ranging from 800 to 999;
- Any inpatient services were rendered.
In ordinary circumstances the form will be sent with a pre-addressed envelope which must then be used to return the completed form to a regional TRICARE office. If an envelope is not included with the paperwork, the DD 2527 must be sent to one of the addresses according to information below:
- The mailing address for West Region Claims is at Claims Department (ATTN: New Claims), PO Box 7981, Madison, WI 53707-7981. Call 1-800-444-5445 for more information.
The East Region includes the following states and territories: Alabama, Arkansas, Connecticut, Delaware, Florida, Georgia, Illinois, Indiana, Iowa (Rock Island area), Kentucky, Louisiana, Maine, Maryland, Massachusetts, Michigan, Mississippi, Missouri (St. Louis area), New Hampshire, New Jersey, New York, North Carolina, Ohio, Oklahoma, Pennsylvania, Rhode Island, South Carolina,Tennessee, Texas (excluding El Paso area), Vermont, Virginia, West Virginia, Washington DC and Wisconsin.
- Residents of the West Region should send all forms to the Claims Department, P.O. Box 202112, Florence, SC 29502-2112, or call 1-844-866-WEST (9378).
The West Region includes the following: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Iowa (excludes Rock Island arsenal area), Kansas, Minnesota, Missouri (except St. Louis area), Montana, Nebraska, Nevada, New Mexico, North Dakota, Oregon, South Dakota, Texas (southwestern corner including El Paso), Utah, Washington and Wyoming.
- TRICARE For Life Claims in the U.S. and U.S. Territories must be sent to WPS TRICARE For Life, P.O. Box 7890, Madison, WI 53707-7890.
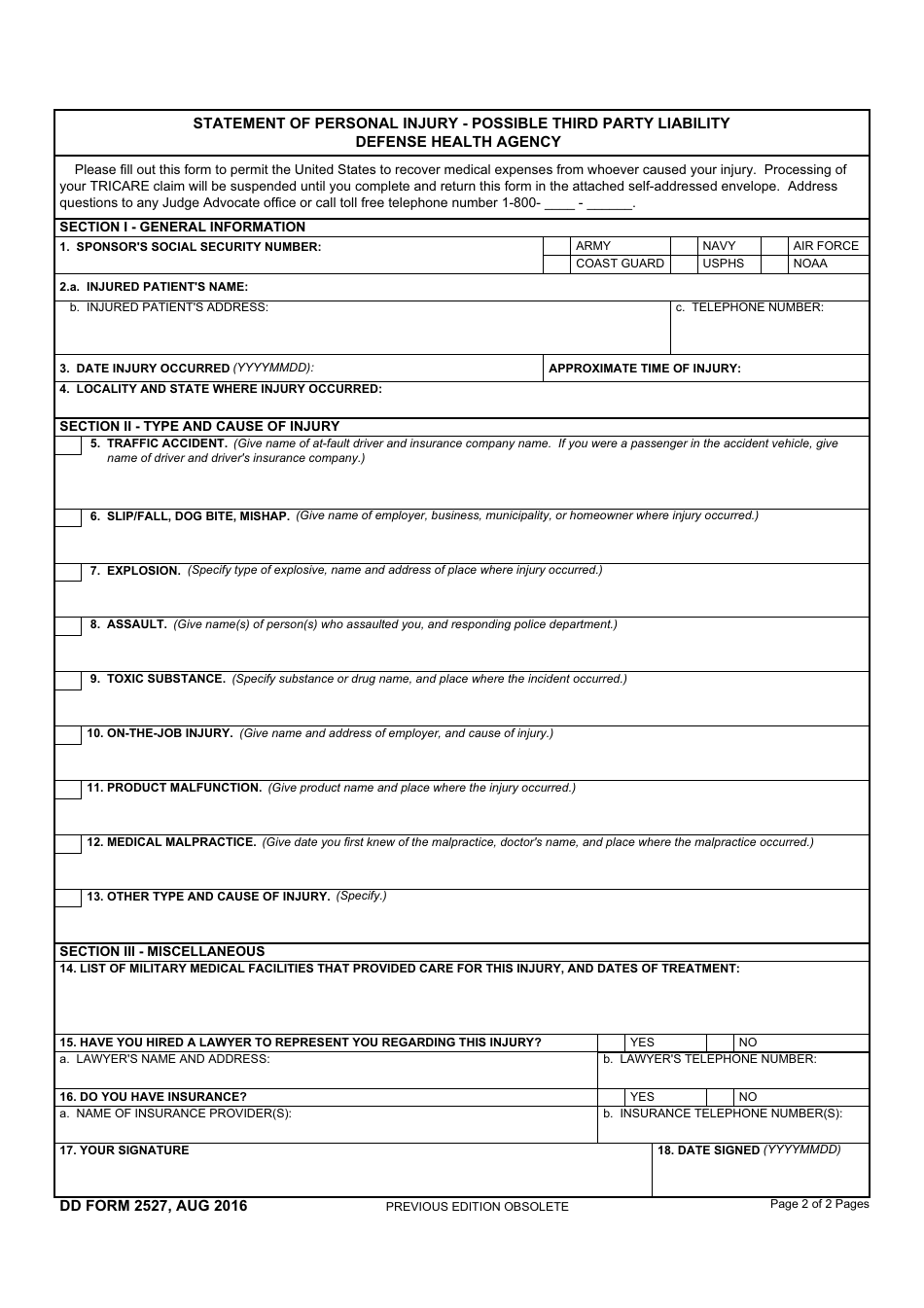
DD Form 2527 Instructions
The form consists of three main sections, a privacy act and an overview of the form. Filing instructions are as follows:
- Section I, General Information, requires specifying the sponsor's SSN, branch of service, name, address and telephone number in Boxes 1 and 2. Boxes 3 and 4 are for providing information about the time, date and place where the injury occured.
- Section II, Type and Cause of Injury, provides nine different options for the applicant to choose out of to classify the cause of the incident or their injury. The provided options include the following:
- Box 5 - Traffic Accident;
- Box 6 - Slip, Fall, Dog Bite or Mishap;
- Box 7 - Explosion;
- Box 8 - Assault;
- Box 9 - Toxic Substance;
- Box 10 - On-the-job Injury;
- Box 11 - Product Malfunction;
- Box 12 - Medical Malpractice;
- Box 13 - Other Type and Cause of Injury.
The individual filing the form must select and file the one box that describes their situation best. The space provided in each of the boxes is for providing the necessary additional details about the injury.
- Section III, Miscellaneous, is made up of four more items. Boxes 14, 15 and 16 are meant for providing specifics and extra information about the accident, medical facilities and available insurance. Box 17 requires the individual to electronically sign the form and specify the date of signing.
Who Signs DD Form 2527?
The DD Form 2527 must be signed by claimant themself in order for the form to be legally valid.
Download DD Form 2527 Statement of Personal Injury - Possible Third Party Liability, Defense Health Agency

1
2