Massachusetts Masshealth Forms
Documents:
79
This form is used for making a sworn statement to verify residency in Massachusetts.
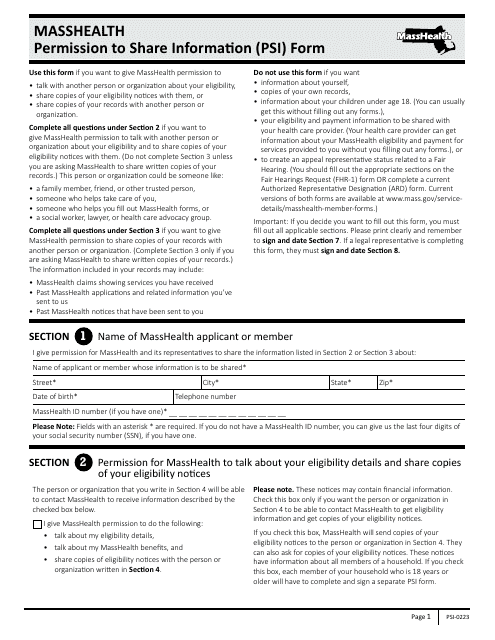
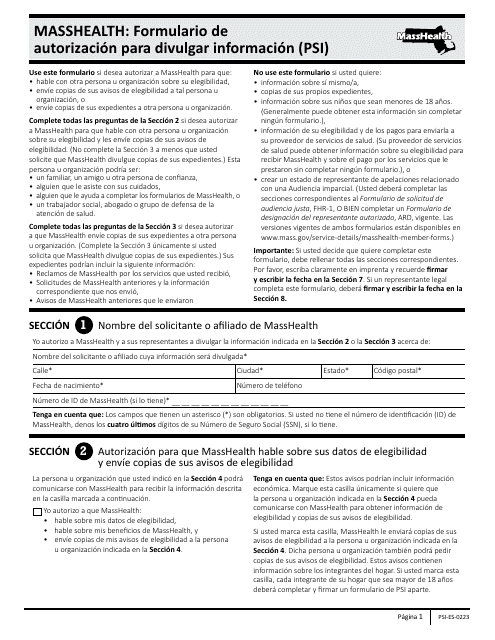
This Form is used for granting permission to share personal information in Massachusetts.
This Form is used for requesting a fair hearing in Massachusetts. It is written in Spanish.
This form is used for applying to the Premium Assistance Program in Massachusetts. It is designed to help individuals and families who meet certain income and eligibility requirements with their health insurance premiums.
This form is used for adults in Massachusetts to apply for disability benefits and provide additional information for their application.
This document is used for authorizing the disclosure of protected health information in Massachusetts.
This Form is used for authorizing the release of protected health information in large print format in Massachusetts.
This type of document is a Spanish form used for requesting reimbursement of pharmacy expenses by mail for MassHealth (Medicaid) members in Massachusetts.
This type of document is for parents in Massachusetts who need to apply for the Disability Supplement for their children through the MassHealth program.
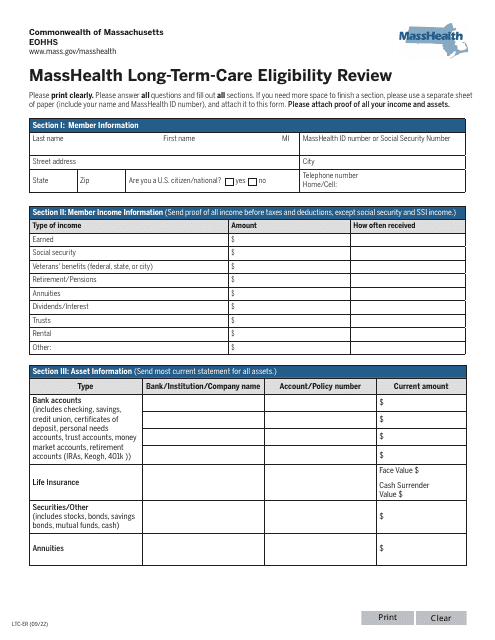
This form is used for the Masshealth Long-Term-Care Eligibility Review in Massachusetts. It is used to determine if individuals are eligible for long-term care services.
This document is used for designating an authorized representative in Massachusetts, in a large print format
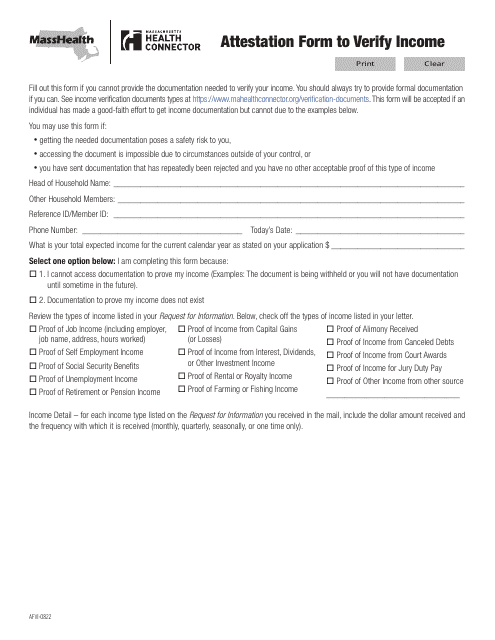
This form is used for individuals in Massachusetts to verify their income through the AFVI Attestation Form.
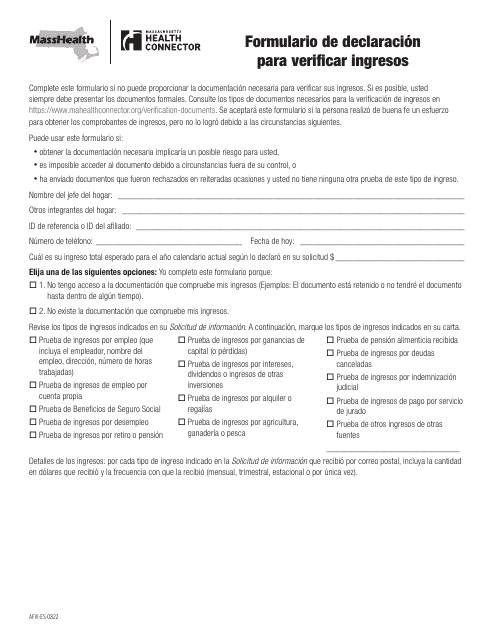
This document is a Form for Income Verification Declaration in Massachusetts. It is used to verify income information.
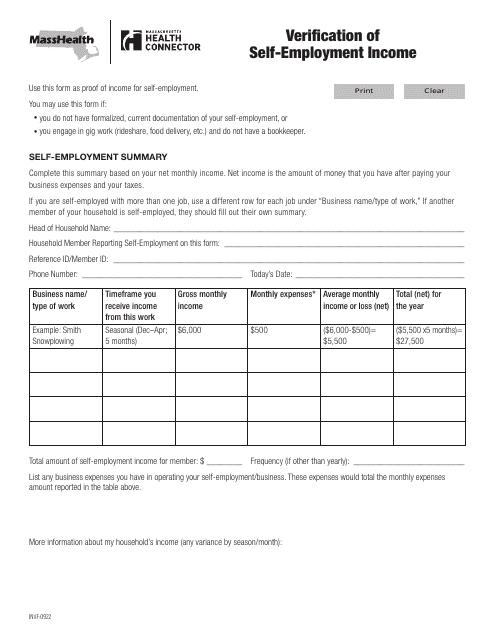
This form is used for verifying self-employment income in Massachusetts.

This Form is used for verifying self-employed income in Massachusetts.
This document is a Spanish form used in Massachusetts for MassHealth. It is a Authorization Form to Disclose Information.
This document allows Masshealth recipients to provide permission for the sharing of their information in a large print format.
This Form is used for requesting reimbursement for pharmacy mail order expenses for MassHealth members in Massachusetts.