California Department of Health Care Services Forms
Documents:
1049
This form is used for obtaining consent for Medi-Cal services in California. It is available in Vietnamese language for the convenience of Vietnamese-speaking individuals.
This form is used for giving consent for Medi-Cal services in California. It is available in Tagalog language.
This document is a consent form for Medi-Cal in California. It is written in Spanish.
This document is used for obtaining written consent for Medi-Cal benefits in California. It is available in Russian language.
This form is used for obtaining consent for Medi-Cal services in California. It is translated into Korean to accommodate individuals who speak Korean as their primary language.
This form is used for obtaining consent for Medi-Cal services in California for individuals who speak Cambodian.
This form is used for obtaining consent for Medi-Cal services in California from individuals who speak Hmong.
This form is used for obtaining consent for Medi-Cal services in California from individuals who speak Farsi.
This Form is used for obtaining consent for Medi-Cal services in California in Chinese.
This form is used for obtaining consent for Medi-Cal services in California from individuals who speak Armenian.
This document is a Medi-Cal Consent Form used in California for Arabic speakers. It allows individuals to give their consent for specific medical procedures or treatments while receiving Medi-Cal benefits.
This form is used for obtaining consent from Medi-Cal beneficiaries in California. It allows the individual to authorize the release of their medical information for certain purposes.
This form is used for updating disability listings in the state of California.
This Form is used for requesting eligibility limited services in the state of California. It serves as a formal request for specific services, indicating the eligibility criteria that need to be met in order to qualify for those services.
This form is used for documenting the therapy sessions and progress of patients in California. It helps healthcare providers keep track of the treatment provided to their patients.
This form is used for submitting a detailed narrative sheet for reporting incidents or providing additional information in the state of California.
This form is used for applying for a financial card in California.
This form is used for summarizing information related to the Medical Therapy Unit (MTU) in California.
This form is used for the Share-Of-Cost Medi-Cal Provider Letter in California. It provides information and instructions for healthcare providers regarding the Medi-Cal program and the share of cost calculations.
This form is used for requesting Medi-Cal coverage for additional family members in California. It is available in Vietnamese.
This form is used for requesting Medi-Cal benefits for additional family members in California. It is available in Tagalog language.
This form is used for adding additional family members who are applying for Medi-Cal in California. It is available in Spanish.
This document is a form used in California for requesting additional family members to be included in a Medi-Cal (Medicaid) application. It is available in the Russian language.
This Form is used for requesting Medi-Cal coverage for additional family members in California. It is available in Korean.
This form is used to request coverage for additional family members under the Medi-Cal program in California for Cambodian residents.
This form is used for requesting Medi-Cal for additional family members in California. It is available in Hmong language.
This form is used for requesting additional family members to be included in the Medi-Cal program in California. It is available in Farsi.
This Form is used for requesting additional family members to be included in your Medi-Cal coverage in California. The form is available in Chinese.
This Form is used for requesting additional family members to be added to your Medi-Cal coverage in California. It is available in Armenian language.
This document is a form for individuals in California who want to add additional family members to their Medi-Cal coverage.
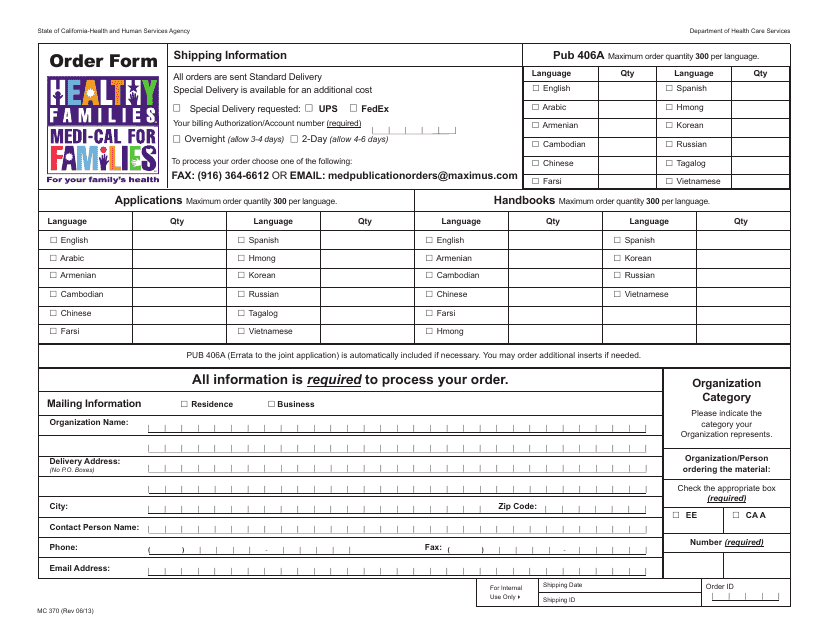
This form is used for ordering the application form for the Healthy Families/Medi-Cal Joint Application in California.
This form is used for providing supplemental information for express enrollment in Medi-Cal, Healthy Families, and Healthy Kids programs in California.
This Form is used for submitting additional information for Express Enrollment applicants in California who speak Russian.
This type of document is used for notifying Hmong applicants in California about a supplemental form required for express enrollment.
This form is used for making a waiver referral to the California Department of Aging (CDA).
This form is used for transmitting a county summary in the state of California. It is used to provide a summary of various documents and information pertaining to a county.
This form is used for transmitting information from Medi-Cal to Healthy Families in California. It allows for the transfer of relevant documents and data between these two healthcare programs.
