Fill and Sign Wisconsin Legal Forms
Documents:
5190
This Form is used for consenting to disqualification in Wisconsin, written in Chinese.
This Form is used for consenting to disqualification in Wisconsin for Russian speakers.
This Form is used for individuals of Hmong descent in Wisconsin who are disqualified from certain programs and wish to enter into a consent agreement to regain eligibility.
This form is used for conducting a device inspection by mail in Wisconsin.
This form is used for applying to the Wisconsin Hemophilia Home Care Program.
This Form is used for certifying the need for specialized medical vehicle transportation in the state of Wisconsin.
This form is used for consenting to a disqualification agreement in Wisconsin for individuals who speak Arabic.
This Form is used for individuals in Wisconsin who have been disqualified from receiving certain benefits and wish to enter into a consent agreement to potentially regain eligibility.
Este formulario se utiliza para registrar el acuerdo de consentimiento de descalificación en el estado de Wisconsin.
This Form is used for requesting prior authorization for brand medically necessary attachments in Wisconsin. It is required to ensure coverage for specific medications deemed medically necessary.
This form is used for filing a HIPAA privacy complaint with the Wisconsin Chronic Disease Program (WCDP) in Wisconsin.
This form is used for reporting and determining the cause of death for clients, patients, or residents in Wisconsin.
Este formulario se utiliza para solicitar un reembolso del programa EWIC en Wisconsin.
This Form is used for applying for initial certification of Community Substance Abuse Services (CSAS) Day Treatment Service in Wisconsin, as per Chapter DHS 75.12.
This document is a Repayment Agreement form for participants in the Wisconsin Ewic Program who speak Hmong. It is used to outline the terms and conditions for repaying any benefits received from the program.
This document is a notice for an administrative disqualification hearing in Wisconsin. It is written in Arabic.
This form is used for requesting reimbursement for nurse aide training and competency test in Wisconsin.
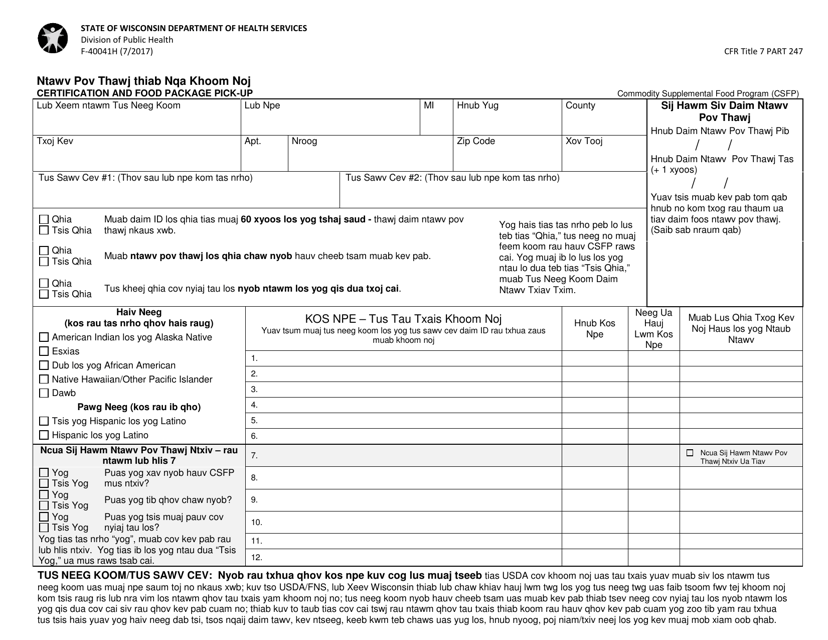
This form is used for certifying eligibility and picking up food packages in Wisconsin specifically for the Hmong community.
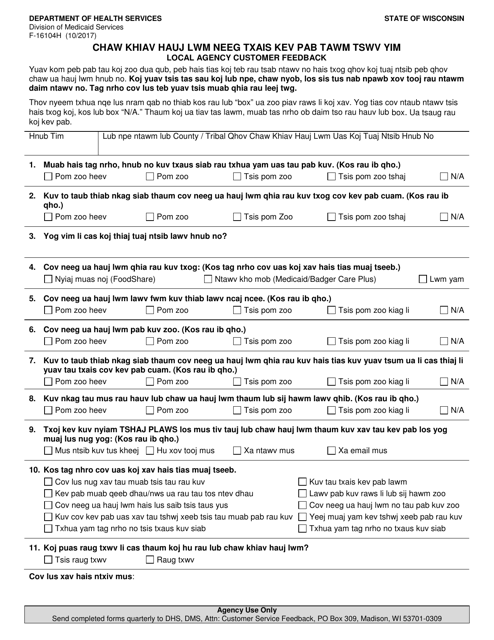
This Form is used for gathering customer feedback from local agencies in Wisconsin, specifically for the Hmong community.
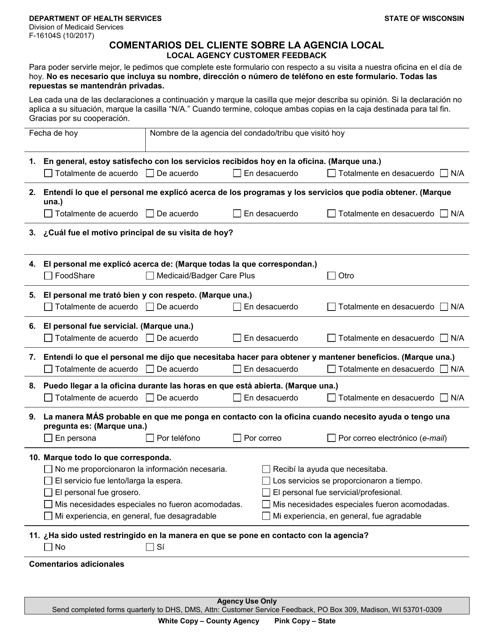
Este formulario se utiliza para que los clientes puedan enviar sus comentarios sobre la agencia local en Wisconsin.
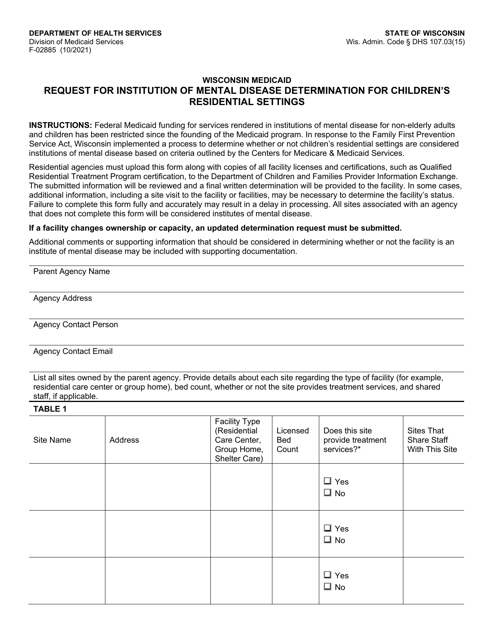
This form is used for requesting a determination of mental disease for children's residential settings in Wisconsin. It is important for ensuring appropriate care and support for children with mental health needs.
This document is used for providing notice of an administrative disqualification hearing in Wisconsin. It is in Spanish.
This document is used for authorizing the disclosure of confidential information for various programs in Wisconsin such as Medicaid, Badgercare Plus, Foodshare, Family Planning Only Services, Seniorcare, and Caretaker Supplement. (Spanish version)
This Form is used for authorizing the release of confidential information in Wisconsin for programs like Wisconsin Medicaid, Badgercare Plus, Foodshare, Family Planning Only Services, Seniorcare, and Caretaker Supplement. It is available in the Hmong language.
This form is used for certifying eligibility and picking up food packages in Wisconsin for Russian-speaking individuals.
This form is used for authorizing the release of immunization records in the Wisconsin Immunization Registry for individuals who speak Hindi.
This type of document is a pregnancy questionnaire for the Prenatal Care Coordination Program in Wisconsin. It is used to collect information about the pregnancy and coordinate prenatal care.
This form is used for collecting important information about a pregnant individual's medical history and pregnancy details for prenatal care coordination in the state of Wisconsin. It is specifically designed for individuals who speak Hmong.
This form is used for submitting prior authorization for headache agents used in preventative treatment in the state of Wisconsin.
This form is used for requesting prior authorization for lipotropics and omega-3 acids drugs in the state of Wisconsin.
This type of document is used for authorizing the release of immunization records to the Wisconsin Immunization Registry. It is specifically available in Chinese language for the convenience of Chinese-speaking individuals residing in Wisconsin.
