Fill and Sign Wisconsin Legal Forms
Documents:
5190
This form is used to apply for a Musky Clubs Alliance license plate in the state of Wisconsin.
This Form is used for applying for a special license plate in Wisconsin that supports the Nurses Change Lives initiative.
This form is used for applying for a Scouting Alumni License Plate in the state of Wisconsin.
This form is used for applying for a Rocky Mountain Elk Foundation license plate in Wisconsin.
This form is used for applying for a Whitetails Unlimited license plate in Wisconsin.
This form is used for assessing the risk of tuberculosis (Tb) and evaluating symptoms in Wisconsin public school employees.
This Form is used for requesting certification for the Veterans Employment Grant in Wisconsin.
This form is used for applying to the Veterans Employment Grant Program in Wisconsin. It is intended to assist veterans in finding employment opportunities.
This form is used for applying for the Veterans Education Grant in the state of Wisconsin. It is specifically for veterans who are looking to pursue higher education.
This Form is used for requesting certification for the Wisconsin G.I. Bill in Wisconsin.
This Form is used for applying for a fee waiver for professional or occupational licensure in Wisconsin.
This Form is used for veterans applying to a Veterans Home in Wisconsin to declare their residency.
This form is used for authorizing the release of income tax information in the state of Wisconsin.
This Form is used for requesting verification of employment in the state of Wisconsin. It is used by individuals who need to provide evidence of their employment for various purposes such as loan applications or immigration proceedings.
This form is used for applying for admission to the Wisconsin Veterans Home in Wisconsin.
This form is used for personal care screening in Wisconsin. It is called the Personal Care Screening Tool (PCST) and has the designation F-11133.
This form is used for obtaining a certificate of status or simple/certified copywork in the state of Wisconsin. It is required for various legal and business purposes.
This form is used for requesting a state fair hearing in Wisconsin.
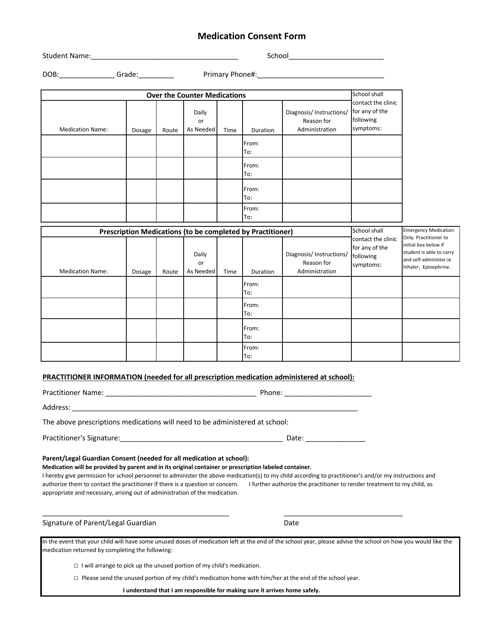
This document is used for obtaining consent for medication administration in the state of Wisconsin.
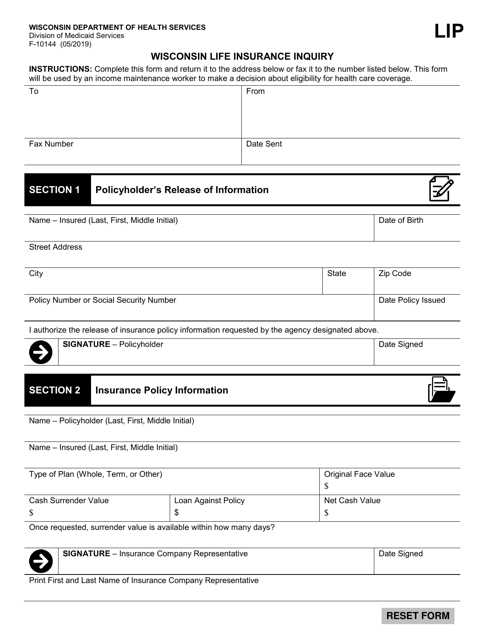
This form is used for making inquiries related to life insurance in the state of Wisconsin
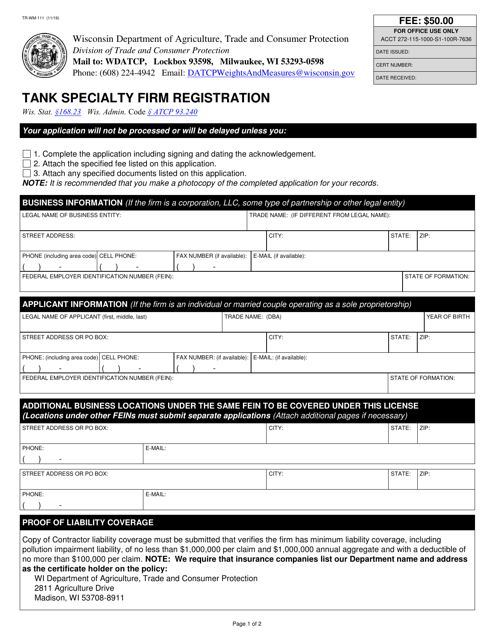
This form is used for tank specialty firms in Wisconsin to register their business.
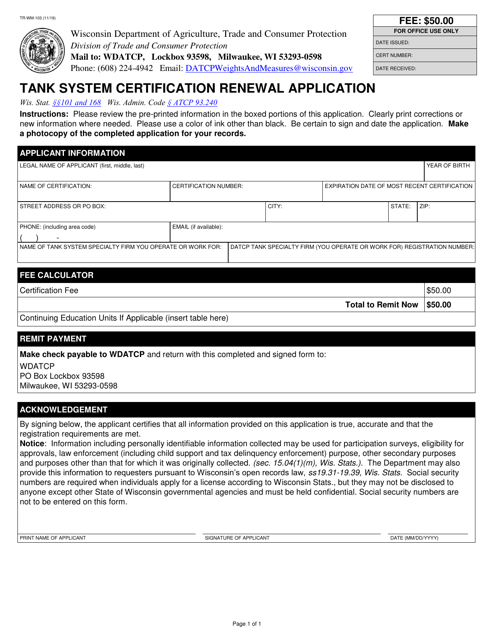
This Form is used for renewing the certification of tank systems in Wisconsin.
This form is used for applying for a corrosion expert certification in Wisconsin.
This form is used for applying for certification as a tank system remover-cleaner in the state of Wisconsin.
This form is used for applying for certification to conduct tank system tightness testing in the state of Wisconsin.
This form is used for applying for certification as an underground tank system installer in Wisconsin.
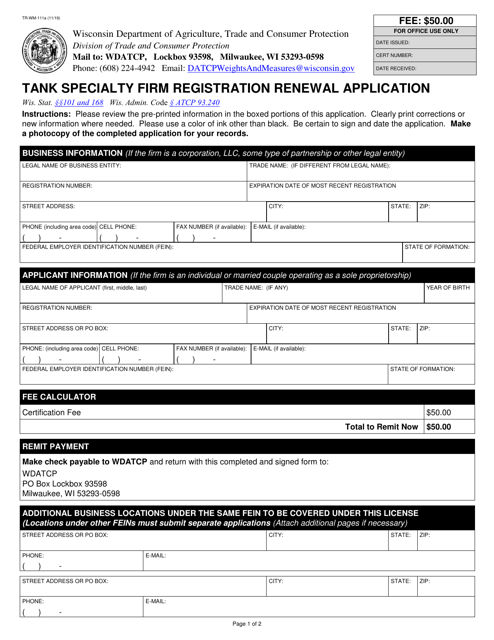
This Form is used for renewing the registration of tank specialty firms in Wisconsin.
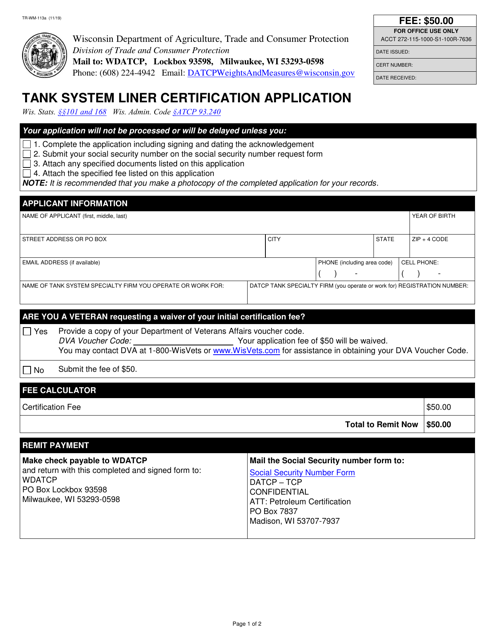
This Form is used for applying for certification of tank system liners in Wisconsin.
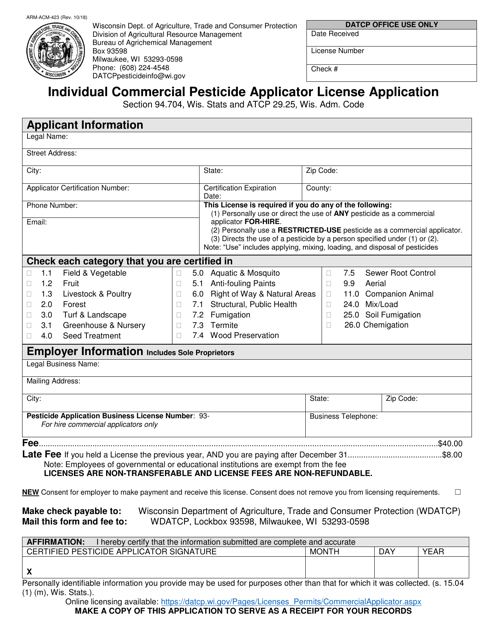
This form is used for individuals in Wisconsin to apply for a commercial pesticide applicator license.
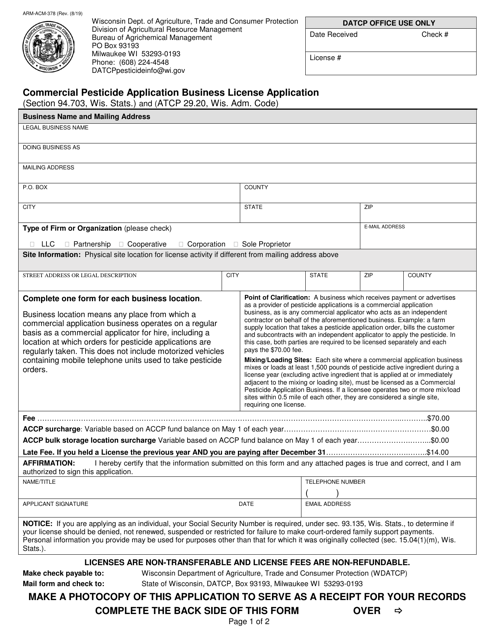
This form is used for applying for a commercial pesticide application business license in Wisconsin.
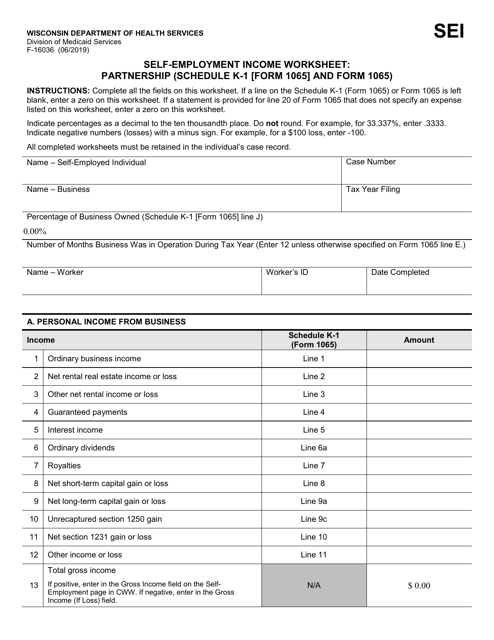
This form is used for calculating self-employment income from a partnership in Wisconsin. It requires information from Schedule K-1 (Form 1065) and Form 1065.
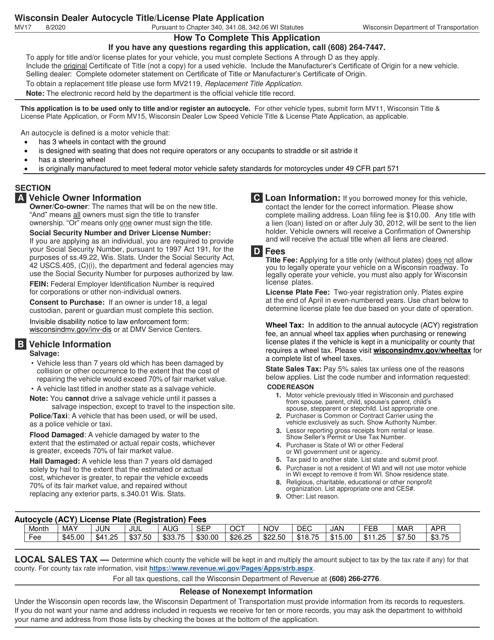
This Form is used for applying for a dealer autocycle title and license plate in Wisconsin.
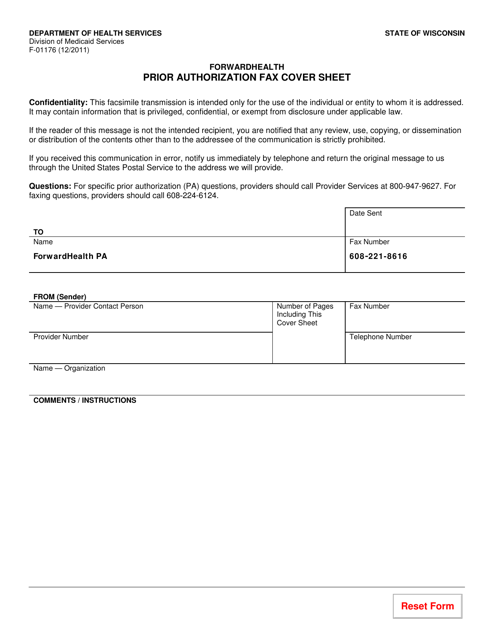
This Form is used for submitting a prior authorization request to Wisconsin's healthcare system. The fax cover sheet must be filled out and attached to the prior authorization form to ensure proper processing.
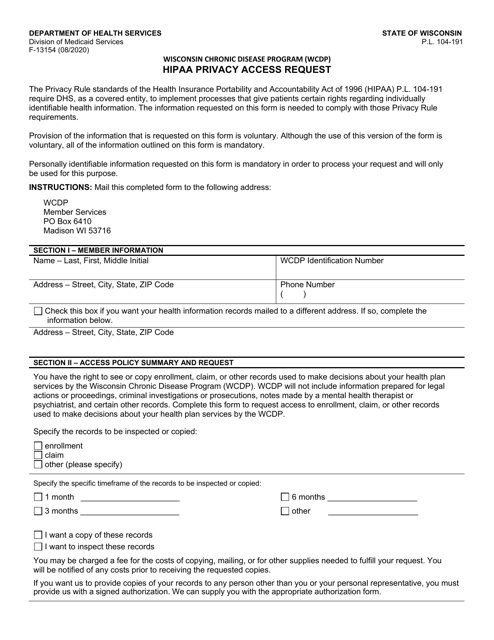
This form is used for requesting access to health information under the Wisconsin Chronic Disease Program (WCDP) in accordance with the HIPAA Privacy Rule.
This form is used for requesting a HIPAA privacy amendment for the Wisconsin Chronic Disease Program (WCDP) in Wisconsin. It allows individuals to make changes or updates to their personal health information in the program.
This form is used for requesting amendments or changes to your protected health information in the Wisconsin Chronic Disease Program (WCDP) under the HIPAA Privacy Rule.
This form is used for requesting alternate communication preferences for the Wisconsin Chronic Disease Program (WCDP) under the guidelines of HIPAA Privacy.
This Form is used for authorizing the use or disclosure of personal health information under the Wisconsin Chronic Disease Program (WCDP) in accordance with HIPAA privacy regulations.
