Workers Compensation Forms and Templates
Documents:
901
This form is used for reporting the first injury that occurred at the workplace in the state of Colorado.
This Form is used for the general admission of liability in workers' compensation cases in Colorado. It helps to determine responsibility for an injury or illness related to work.
This form is used for notifying the employer and insurance company in Colorado about a one-time change of physician and authorizing the release of medical information.
This Form is used for the monthly summary of workplace injury and illness data in the state of Colorado.
This Form is used for providing a settlement routing sheet in the state of Colorado.
This document is for employers in Alaska to report 45 consecutive days of time loss for injuries suffered by their employees.
This Form is used for employers in Alaska to provide notice of 90 consecutive days of time loss for injuries suffered by an employee. It is important for employers to fill out this form accurately and submit it to the appropriate authorities.
This Form is used for providing workers' compensation carrier information in the state of Florida.
This form is used for physicians in Connecticut to report on the workers' status.
This form is used to request a change of physician in the state of Colorado.
This form is used for workers' compensation and leave without pay claim and verification in Alaska.
This Form is used for Wage Statement purposes in the state of Florida. It is a document that reports an employee's wages and other compensation.
This form is used for submitting a Claim Cost Report in the state of Florida. It is required to report and document the costs associated with a claim.
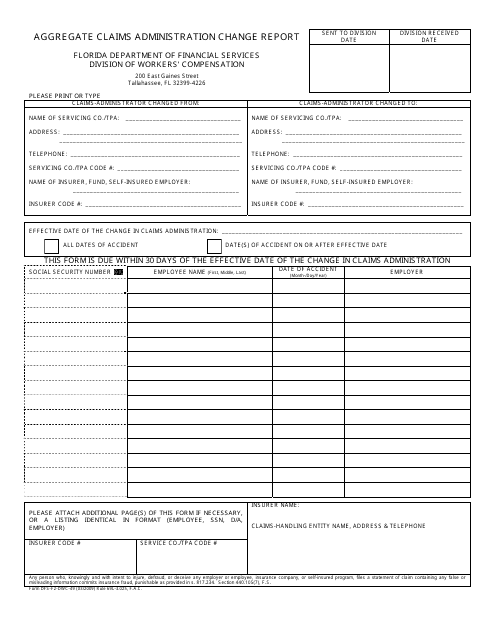
This form is used for reporting changes in aggregate claims administration in the state of Florida.
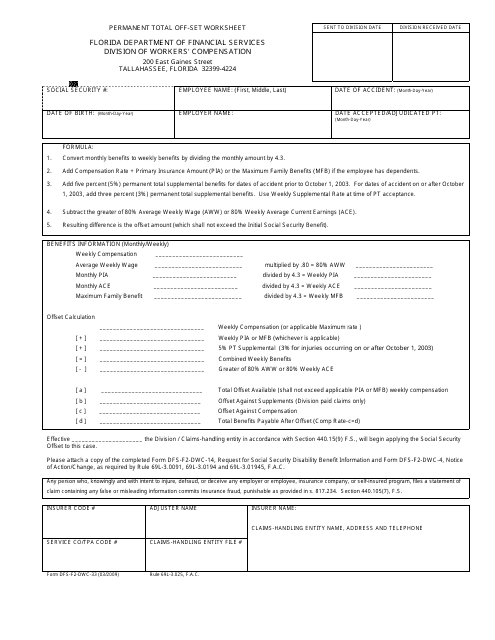
This form is used in Florida for calculating permanent total offset benefits in workers' compensation cases.
This Form is used for workers in Alaska to claim for Workers' Compensation Benefits.
This form is used for filing a workers' compensation claim and providing verification in the state of Alaska.
This form is used for submitting workers' compensation documents to the relevant authorities in Arizona. It is specifically designed for individuals or organizations who are considered interested parties in a workers' compensation case.
This Form is used for workers in Arizona to report an injury that occurred while on the job.
This Form is used for employers in Arizona to report industrial injuries suffered by their employees.
This Form is used for employees in Arizona to notify their employer of their rejection of the terms of the Arizona Workers' Compensation Law.
This form is used for filing a complaint against an employer in Arizona who does not have workers' compensation insurance.
This Form is used for notifying the carrier about a scheduled injury in the state of Arizona.
This document is used by carriers to be notified of a scheduled injury in Arizona.
This type of document is used to inform the carrier about a scheduled injury in Arizona.
This form is used for employers to respond to inquiries regarding workers' compensation insurance in Arizona.
This document is used for filing a supplemental claim for compensation for workers in the state of Arizona. It allows workers to request additional compensation for work-related injuries or illnesses.
This Form is used for reporting a worker's injury in Arizona. It requires information from both the worker and the physician involved.
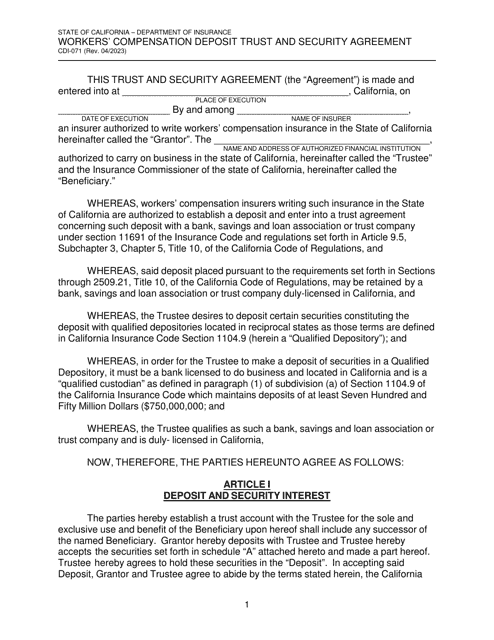
This document is used for guaranteeing workers' compensation liabilities in the state of California.
This Form is used for authorizing a corporate resolution to apply for a Certificate of Consent to self-insure workers' compensation liabilities in the State of California.
This Form is used for the agreement of assumption and guarantee of workers' compensation liabilities for group and affiliate members in California.
This form is used for requesting a letter of credit in order to make a deposit for workers' compensation in California.
This Form is used for reporting respiratory diseases in the state of Connecticut.
This form is used for reporting the first occurrence of an injury or illness in the state of Florida. It is important to complete and submit this form as soon as possible after the incident.
This form is used for revoking the election of coverage in the state of Florida. It allows individuals to withdraw from the coverage they had previously elected.
This form is used for the Board of Equalization of Compensation in Alabama to address issues related to compensation.
This form is used for Alabama employers who wish to apply for self insurance for workers' compensation coverage.