Health Insurance Form Templates
Documents:
681
This document is used for deferring the enrollment in the NYSHIP health insurance plan in New York.
This Form is used for requesting prior authorization for the medication Orilissa (Elagolix) in the state of Nevada.
This form is used for reimbursement of non-emergency medical travel expenses in South Dakota. It is specifically for the Non-Emergency Medical Travel (NEMT) program.
This form is used for notifying individuals in Texas about actions taken regarding their Medicaid benefits.
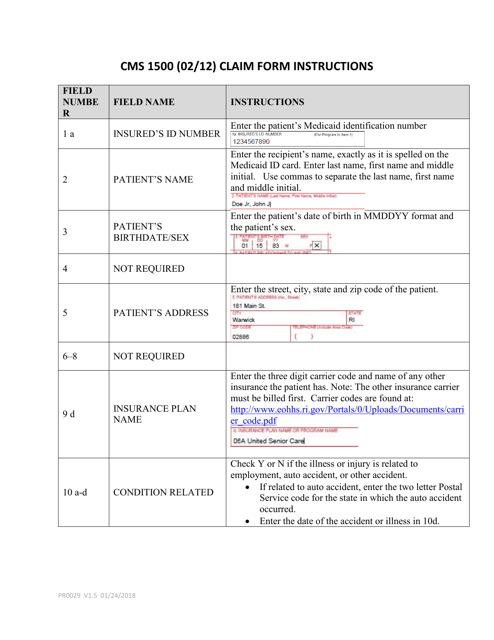
This form is used for submitting healthcare claims to the State Health Plan in South Carolina.
This document outlines the self-insured employer's plan for managed care in South Dakota. It provides information on how employers can provide healthcare coverage to their employees through a managed care system.
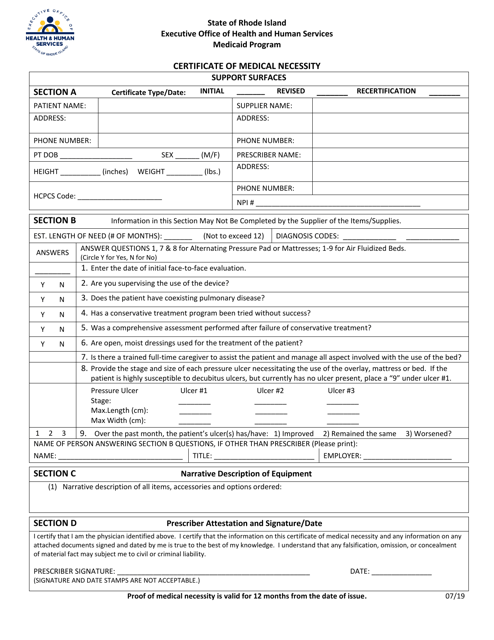
This Form is used for obtaining a Certificate of Medical Necessity for Pressure Reducing Support Surfaces in Rhode Island. It is required to be filled out by a healthcare provider to justify the need for this type of equipment for a patient's medical condition.
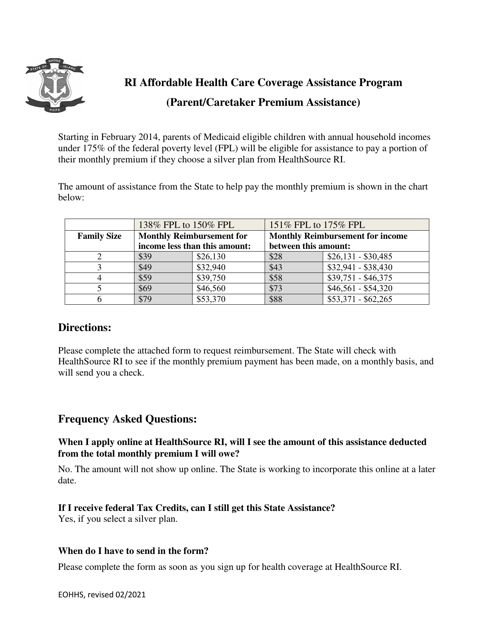
This form is used for applying for state-funded assistance in Rhode Island to help pay for health care coverage.
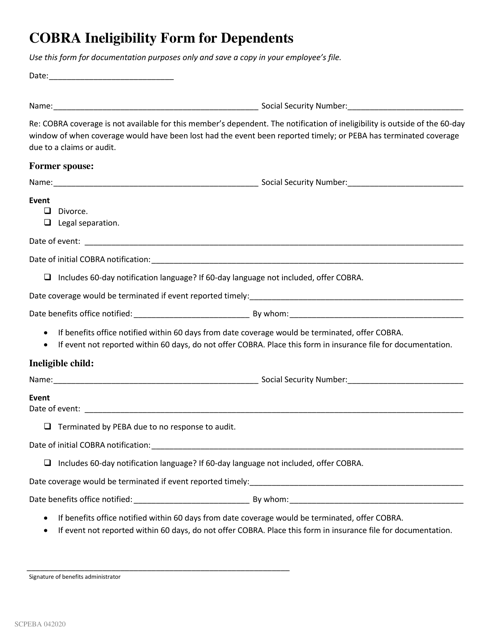
This form is used for dependents who are ineligible for Cobra coverage in South Carolina.
This document is a notice regarding a qualifying event for COBRA in South Carolina. COBRA refers to the Consolidated Omnibus Budget Reconciliation Act, which provides temporary continuation of group health coverage in certain situations. The notice informs individuals of a qualifying event that may entitle them to COBRA coverage.
This document is a notice informing individuals in South Carolina about an extension of their COBRA continuation coverage. COBRA allows people to maintain their health insurance coverage after certain qualifying events, such as job loss or reduction in work hours.
This document is an application for a Medicare Advantage Prescription Drug (MAPD) plan for residents of Oklahoma. It is used to apply for a healthcare plan that provides both prescription drug coverage and additional benefits beyond what is offered by Original Medicare.
This Form is used for applying for a Medicare Supplement plan that includes prescription drug coverage in the state of Oklahoma.
This document explains the coverage that Medicare provides for healthcare services received outside of the United States. It includes information on the limitations and requirements for receiving medical care abroad under Medicare.
This document is for understanding Medicare coverage outside of the United States. It provides information on what medical services are covered and the limitations of coverage when traveling or living abroad.
This document is used for obtaining prior authorization for the medication Valganciclovir Hydrochloride (Valcyte) in the state of Illinois.
This form is used for petitioning to change your primary treating physician in California's workers' compensation system.
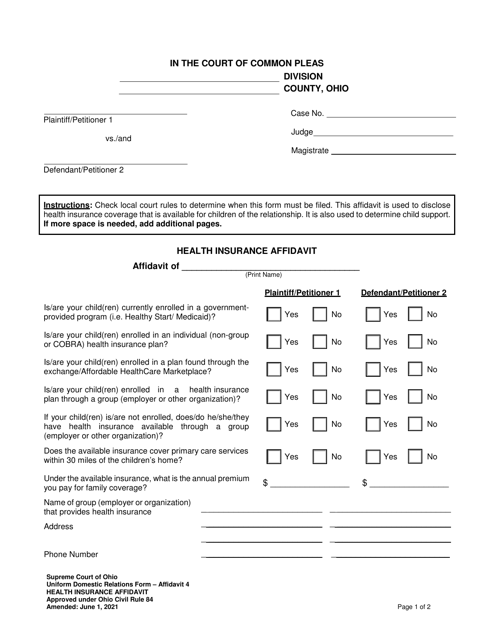
This form is used for requesting health insurance information in the state of Ohio.
This form is used for providing health insurance information in the state of Ohio.
This form is used for applying for the Healthcare Evidence Initiative for your own household in the state of California.
Individuals can use this type of document as a reference when they would like to claim a use for their medical insurance.
This is a document that you can use if you would like to appeal a decision made by your insurance company to deny your medical claim.
Individuals may use a letter such as this as a reference when they would like to request a copy of their records from a medical organization where they have been treated.
This Form is used for filing a claim for medical reimbursement from the Office of Workers' Compensation Programs (OWCP). It is used by individuals seeking compensation for their medical expenses related to a work-related injury or illness.
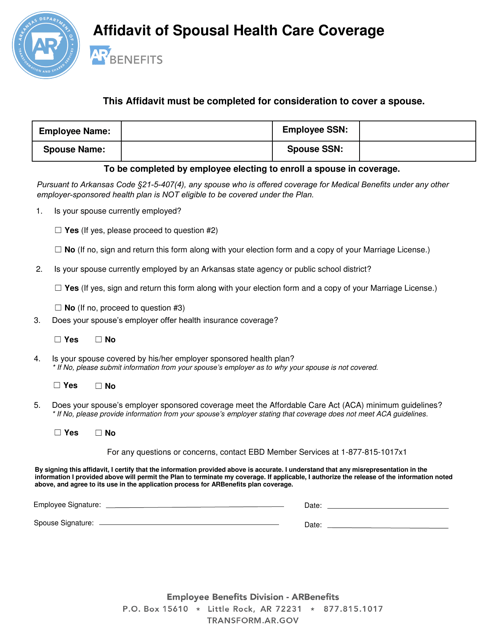
This form is used for declaring the health care coverage of a spouse in Arkansas.

This form is used for applying for health insurance in California.