Coordinated Care Templates
Are you in need of well-coordinated and comprehensive healthcare services? Look no further than our Coordinated Care program. We understand that navigating the healthcare system can be overwhelming, which is why we have developed a range of services to ensure that you receive the care you need, when you need it.
Our team of experienced Care Coordinators are dedicated to working closely with you and your healthcare providers to create a seamless healthcare experience. From managing your healthcare transitions to ensuring that you have access to the right resources and support, our Care Coordinators are here to make the process as smooth as possible.
Our Coordinated Care program offers a variety of services, including the Continuity of Care Acute Care Transfer Form - Rhode Island and the Transition of Care Form - West Virginia. These forms are designed to capture all the necessary information about your health and ensure that it is accurately communicated between different healthcare providers, promoting continuity and avoiding any gaps in your care.
In addition, our program includes the Form CERT-47 Individual Care Coordinator Conflict of Interest Assurance - Alaska and the 1915(I) Care Coordination Request Report - North Dakota. These documents are essential for maintaining transparency and accountability in the care coordination process, ensuring that your best interests are always the priority.
Our commitment to coordinated care extends beyond geographical boundaries. That's why we are also proud to offer the Form WNSCA027 Warwickshire North Shared Care Agreement - United Kingdom, providing cross-border care coordination for individuals who require healthcare services while travelling or residing in the United Kingdom.
At our core, we believe that coordinated care is key to achieving the best possible health outcomes for our patients. With our comprehensive range of services and dedicated team of Care Coordinators, we are here to support you every step of the way. Leave the complexities of managing your healthcare to us, so you can focus on what matters most - your health and well-being.
Documents:
28
This document is a guide that provides information on Medicare Special Needs Plans (SNPs). It explains what SNPs are and the benefits they offer for individuals with specific health needs. It also highlights the eligibility criteria and enrollment process for SNPs.
This document is used for creating a shared plan of care for healthcare providers in Colorado. It helps coordinate and communicate the patient's care among various providers.
This form is used for referring individuals in New Jersey to long-term services and supports. It helps assess their eligibility and needs for assistance with daily activities and healthcare services.

This checklist is used for managed care organizations operating in the state of Delaware. It includes requirements and guidelines for compliance and best practices in managing care for patients.
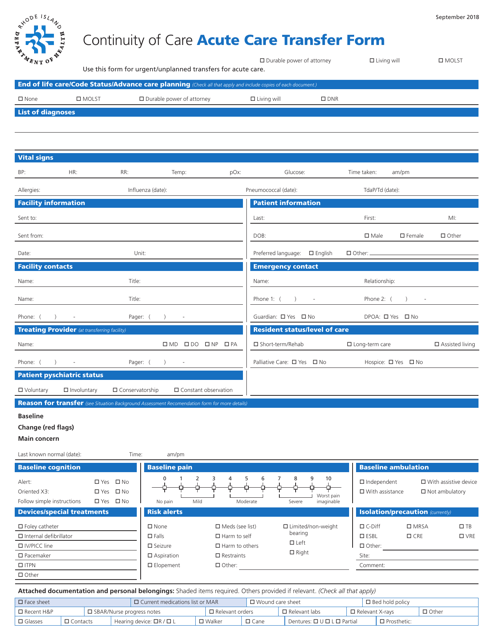
This document is used for transferring patients between acute care facilities in Rhode Island while ensuring continuity of care.
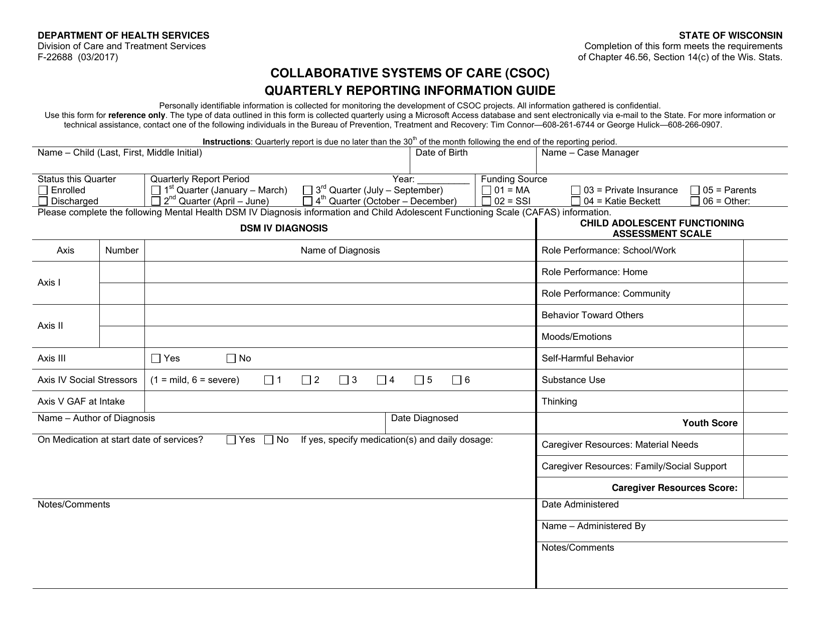
This document provides guidance and information for completing the Collaborative Systems of Care (Csoc) Quarterly Reporting for Wisconsin.
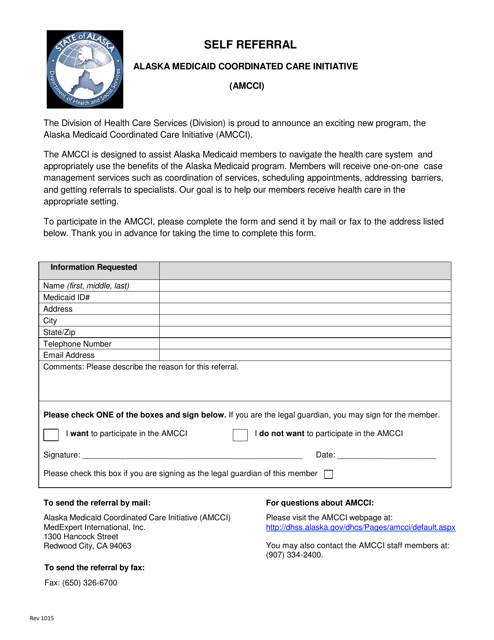
This type of document allows individuals in Alaska to refer themselves to the Medicaid Coordinated Care Initiative (AMCCI) for coordinated healthcare services.
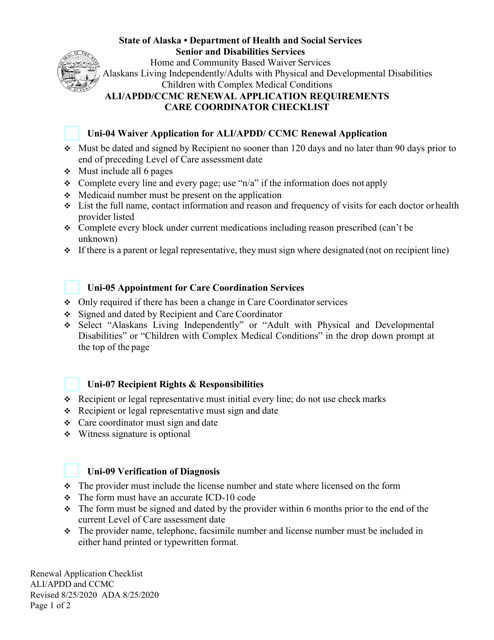
This document provides a checklist of the requirements for renewing an Ali/Apdd/Ccmc Care Coordinator certification in Alaska. It outlines the necessary documents and steps needed to complete the renewal process.
This form is used for reporting changes in care coordinator information in the state of Alaska.
This form is used for referring individuals to the Medicaid Health Home program in South Dakota.
This Form is used for referring patients to care coordination services in Utah. It helps facilitate communication and collaboration among healthcare providers to ensure patients receive appropriate and timely care.
This type of document provides answers to common questions regarding Transitional Care Management. It is a resource provided by the American Academy of Family Physicians.
This Form is used for creating a Family Support Plan for Single Agency Care Coordination in the state of Florida. It is a document that helps families in need of support services to develop a plan for coordinating their care with a single agency.
This document is for those seeking a referral for home care services in Prince Edward Island, Canada. It provides information and assistance in finding reliable and professional home care providers in the area.
This document is used for facilitating the transition of care for patients in West Virginia. It helps to ensure that relevant medical information is accurately and efficiently transferred between healthcare providers.
This Form is used for assessing the multidisciplinary team and person-centered care planning process in California.
This Form is used for coordinating long-term care and hospice services in Missouri.
This document is a care coordination request report specific to North Dakota in the year 1915. It provides information and requests for coordinated care services in the state.
This document is used for obtaining individual acknowledgements and signatures for care coordination in the state of North Dakota.
This document is used for the review of direct care observations conducted by clinicians for clients in North Dakota.
This form is used for making an appointment to receive Care Coordination/Targeted Case Management Services in Alaska.
This document is meant to aid and guide in the creation of a comprehensive plan for transitioning patients from a healthcare facility back to their homes or another type of care facility, ensuring that all their care needs will be met upon discharge.
This form is used for establishing a shared care agreement in Warwickshire North, United Kingdom. It outlines expected standards and responsibilities for both parties involved, ensuring optimal healthcare collaboration.
This document is a checklist used by care coordinators in Alaska to request inquiries about CFC (Child and Family Connections) providers.